Department of Dermatology, Northwestern University Feinberg School of Medicine, Chicago, IL, USA.
Ann and Robert H. Lurie Children's Hospital, Chicago, IL, USA.
Paediatr Drugs. 2024 Mar;26(2):163-173. doi: 10.1007/s40272-023-00611-9. Epub 2024 Jan 24.
Patients with atopic dermatitis (AD), particularly infants and young children, are at greater risk of developing skin infections. In this study, we assessed infection rates in AD patients aged 6 months to 5 years treated with dupilumab.
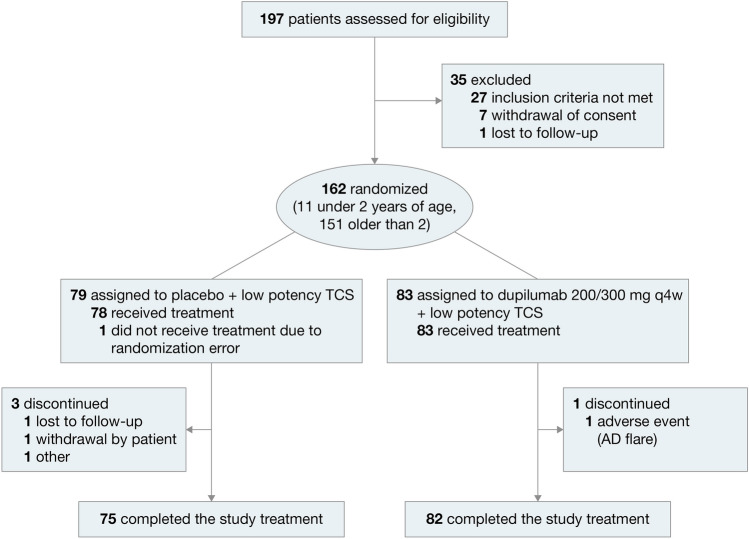
In LIBERTY AD PRESCHOOL, a double-blind, placebo-controlled, phase III clinical trial, children aged 6 months to 5 years with moderate-to-severe AD were randomized 1:1 to subcutaneous dupilumab or placebo, with concomitant low-potency topical corticosteroids, every 4 weeks for 16 weeks. Exposure-adjusted infection rates were used to compare treatment groups.
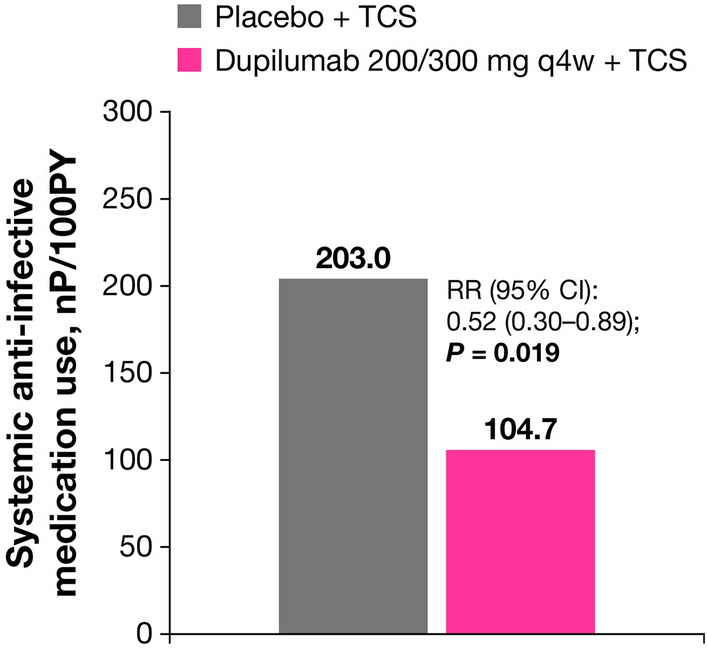
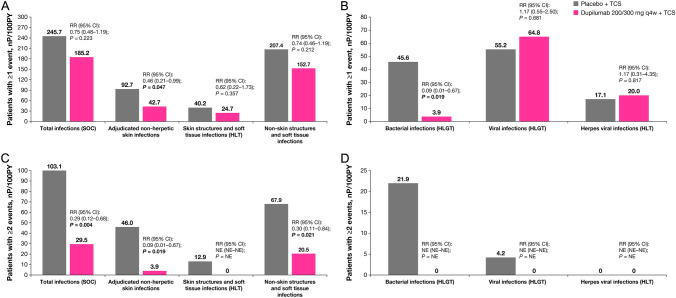
The analysis included 162 patients, of whom 83 received dupilumab and 79 received placebo. Total infection rates were not significantly different between the dupilumab and placebo groups (rate ratio [RR] 0.75, 95% CI 0.48-1.19; p = 0.223). Non-herpetic adjudicated skin infections and bacterial infections were significantly less frequent with dupilumab versus placebo (non-herpetic skin infections: RR 0.46, 95% CI 0.21-0.99; p = 0.047; bacterial infections: RR 0.09, 95% CI 0.01-0.67; p = 0.019), and the number of patients using systemic anti-infective medication was significantly lower in the dupilumab group (RR 0.52, 95% CI 0.30-0.89; p = 0.019). There were no significant differences in the number of herpetic infections between the dupilumab and placebo groups (RR 1.17, 95% CI 0.31-4.35; p = 0.817). The number of patients with two or more infection events was significantly higher in the placebo group (RR 0.29, 95% CI 0.12-0.68; p = 0.004), and no severe or serious infections (including eczema herpeticum) were observed among patients receiving dupilumab.
These data suggest that dupilumab treatment in infants and children younger than 6 years with AD does not increase overall risk of infections and is associated with a reduced risk of bacterial and non-herpetic skin infections compared with placebo, resulting in a reduced need for anti-infective medication.
The trial was registered with ClinicalTrials.gov with ID number NCT03346434 on November 17, 2017. INFOGRAPHIC.
特应性皮炎(AD)患者,尤其是婴儿和幼儿,发生皮肤感染的风险更高。在这项研究中,我们评估了接受度普利尤单抗治疗的 6 个月至 5 岁 AD 患者的感染率。
在 LIBERTY AD PRESCHOOL 这项双盲、安慰剂对照、III 期临床试验中,6 个月至 5 岁中重度 AD 患儿以 1:1 的比例随机分配至度普利尤单抗或安慰剂组,同时接受低效力外用皮质类固醇治疗,每 4 周 1 次,共 16 周。采用暴露调整感染率来比较治疗组。
该分析纳入了 162 例患者,其中 83 例接受度普利尤单抗治疗,79 例接受安慰剂治疗。度普利尤单抗组和安慰剂组的总感染率无显著差异(率比[RR]0.75,95%CI 0.48-1.19;p=0.223)。与安慰剂相比,度普利尤单抗治疗组非疱疹性经裁决的皮肤感染和细菌性感染明显减少(非疱疹性皮肤感染:RR 0.46,95%CI 0.21-0.99;p=0.047;细菌性感染:RR 0.09,95%CI 0.01-0.67;p=0.019),度普利尤单抗组使用全身抗感染药物的患者数量明显减少(RR 0.52,95%CI 0.30-0.89;p=0.019)。度普利尤单抗组和安慰剂组的疱疹性感染数量无显著差异(RR 1.17,95%CI 0.31-4.35;p=0.817)。安慰剂组有 2 次或以上感染事件的患者比例明显更高(RR 0.29,95%CI 0.12-0.68;p=0.004),而接受度普利尤单抗治疗的患者未观察到严重或严重感染(包括疱疹样湿疹)。
这些数据表明,与安慰剂相比,AD 患儿(年龄<6 岁)接受度普利尤单抗治疗并不会增加总体感染风险,并且与降低细菌和非疱疹性皮肤感染风险相关,从而减少对抗感染药物的需求。
该试验于 2017 年 11 月 17 日在 ClinicalTrials.gov 上注册,编号为 NCT03346434。信息图。