Yakdan Salim M, Greenberg Jacob K, Krishnaney Ajit A, Mroz Thomas E, Spiessberger Alexander
Department of Neurological Surgery, Washington University, St. Louis, MO, USA.
Center for Spine Health, Cleveland Clinic, Neurologic Institute, Cleveland, OH, USA.
J Craniovertebr Junction Spine. 2023 Oct-Dec;14(4):393-398. doi: 10.4103/jcvjs.jcvjs_112_23. Epub 2023 Nov 29.
Anterior craniocervical junction lesions have always been a challenge for neurosurgeons. Presenting with lower cranial nerve dysfunction and symptoms of brainstem compression, decompression is often required. While posterior approaches offer indirect ventral brainstem decompression, direct decompression via odontoidectomy is necessary when they fail. The transoral and endoscopic endonasal approaches have been explored but come with their own limitations and risks. A novel retropharyngeal approach to the cervical spine has shown promising results with reduced complications.
This study aims to explore the feasibility and potential advantages of the anterior retropharyngeal approach for accessing the odontoid process.
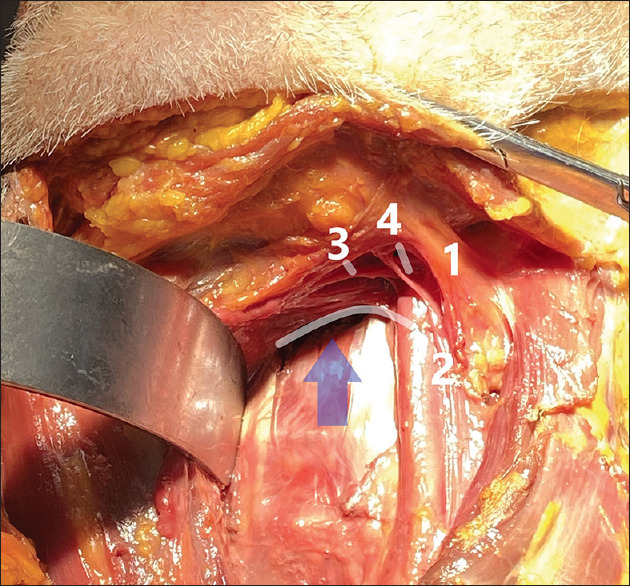
To investigate the anatomical aspects of the anterior retropharyngeal approach, a paramedian skin incision was performed below the submandibular gland on two cadaveric specimens. The subcutaneous tissue followed by the platysma is dissected, and the superficial fascial layer is opened. The plane between the vascular sheath laterally and the pharyngeal structures medially is entered below the branching point of the facial vein and internal jugular vein. After reaching the prevertebral plane, further dissection cranially is done in a blunt fashion below the superior pharyngeal nerve and artery. Various anatomical aspects were highlighted during this approach.
The anterior, submandibular retropharyngeal approach to the cervical spine was performed successfully on two cadavers highlighting relevant anatomical structures, including the carotid artery and the glossopharyngeal, hypoglossal, and vagus nerves. This approach offered wide exposure, avoidance of oropharyngeal contamination, and potential benefit in repairing cerebrospinal fluid fistulas.
For accessing the craniocervical junction, the anterior retropharyngeal approach is a viable technique that offers many advantages. However, when employing this approach, surgeons must have adequate anatomical knowledge and technical proficiency to ensure better outcomes. Further studies are needed to enhance our anatomical variations understanding and reduce intraoperative risks.
颅颈交界区前部病变一直是神经外科医生面临的挑战。患者表现为低位颅神经功能障碍和脑干受压症状,通常需要进行减压手术。虽然后路手术可实现间接的腹侧脑干减压,但当减压失败时,通过齿状突切除术进行直接减压是必要的。经口和内镜鼻内入路已被探索,但都有各自的局限性和风险。一种新颖的经咽后入路治疗颈椎已显示出有希望的结果,并发症减少。
本研究旨在探讨经咽后前路入路到达齿状突的可行性和潜在优势。
为研究经咽后前路入路的解剖学特点,在两个尸体标本的下颌下腺下方做了一个旁正中皮肤切口。依次切开皮下组织和颈阔肌,打开浅筋膜层。在面静脉和颈内静脉分支点下方进入外侧血管鞘和内侧咽部结构之间的平面。到达椎前平面后,在咽上神经和动脉下方钝性向上进一步解剖。在此入路过程中突出了各种解剖学特点。
在两具尸体上成功实施了经咽后前路入路治疗颈椎,突出了相关解剖结构,包括颈动脉以及舌咽神经、舌下神经和迷走神经。该入路提供了广泛的暴露,避免了口咽污染,并在修复脑脊液漏方面具有潜在优势。
对于进入颅颈交界区,经咽后前路入路是一种可行的技术,具有许多优势。然而,采用此入路时,外科医生必须具备足够的解剖学知识和技术熟练程度,以确保更好的手术效果。需要进一步研究以增强我们对解剖变异的理解并降低术中风险。