Patel Arpan, Walling Anne, Kanwal Fasiha, Serper Marina, Hernaez Ruben, Sundaram Vinay, Kaplan David, Taddei Tamar, Mahmud Nadim
Vatche and Tamar Manoukian Division of Digestive Diseases, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States.
Department of Medicine, Greater Los Angeles VA Healthcare System, Los Angeles, CA, United States.
JHEP Rep. 2023 Nov 30;6(2):100976. doi: 10.1016/j.jhepr.2023.100976. eCollection 2024 Feb.
BACKGROUND & AIMS: There is growing acceptance that principles of palliative care should be integrated into the management of serious illnesses affecting the liver, such as acute-on-chronic liver failure (ACLF). However, rates, patterns, and predictors of specialty palliative care consultation among patients with ACLF have not been well-described.
We performed a retrospective cohort study of patients hospitalized with ACLF between 1/1/2008 and 12/31/2018 using the VOCAL cohort. Patients were followed until 6/2021. We used mixed-effects regression analyses to identify significant patient and facility factors associated with palliative care consultation. We examined timing of consultation, the influence of ACLF characteristics, and facility-level variation on receipt of palliative care consultation.
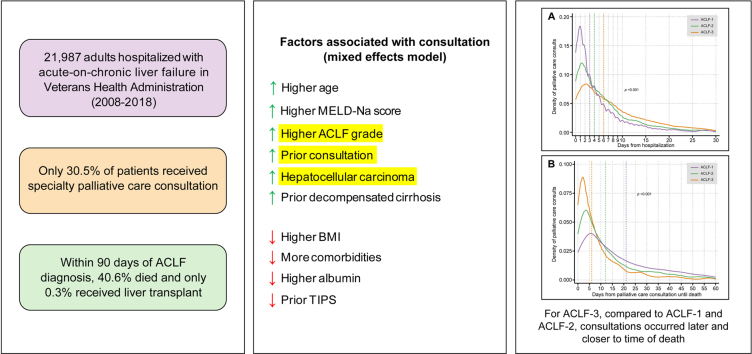
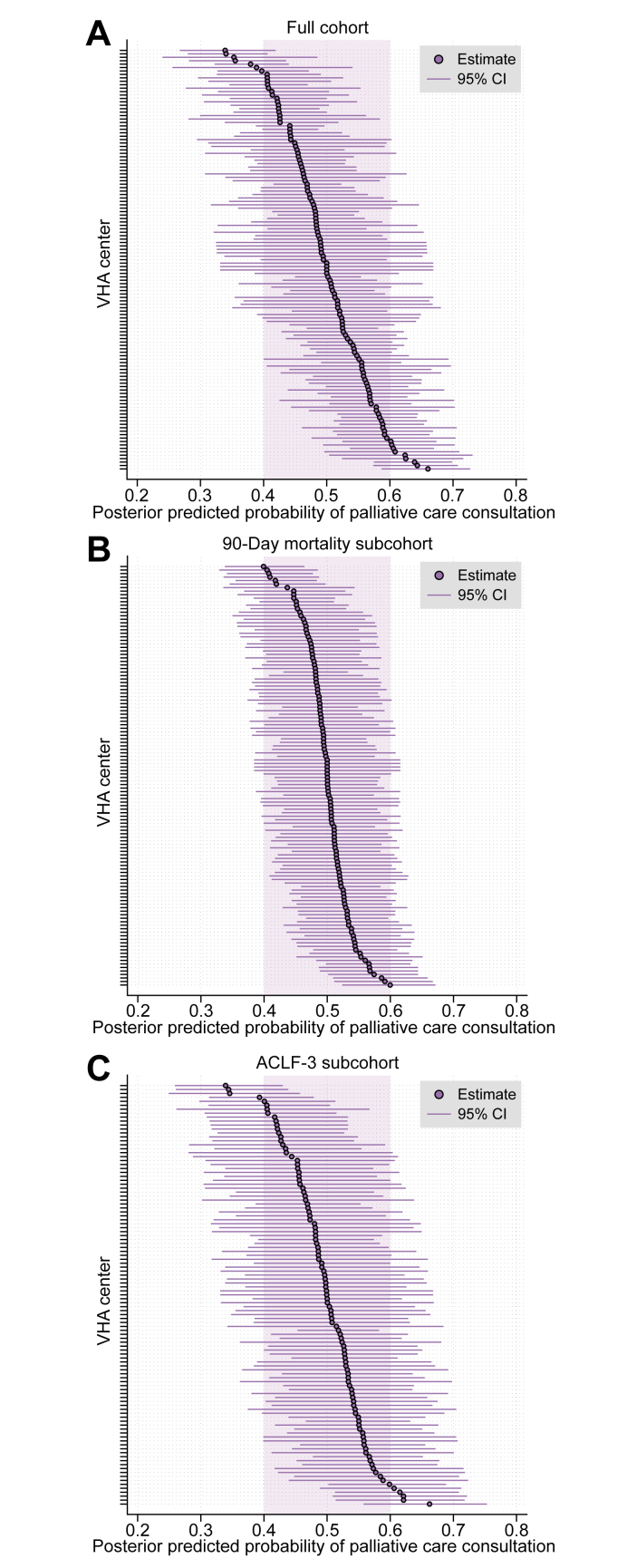
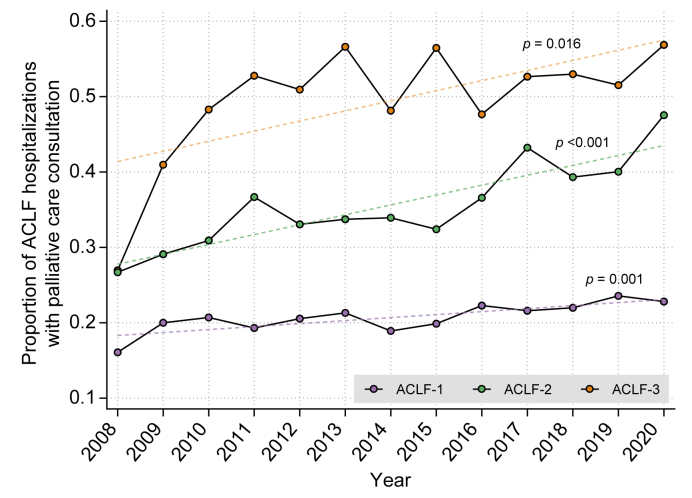
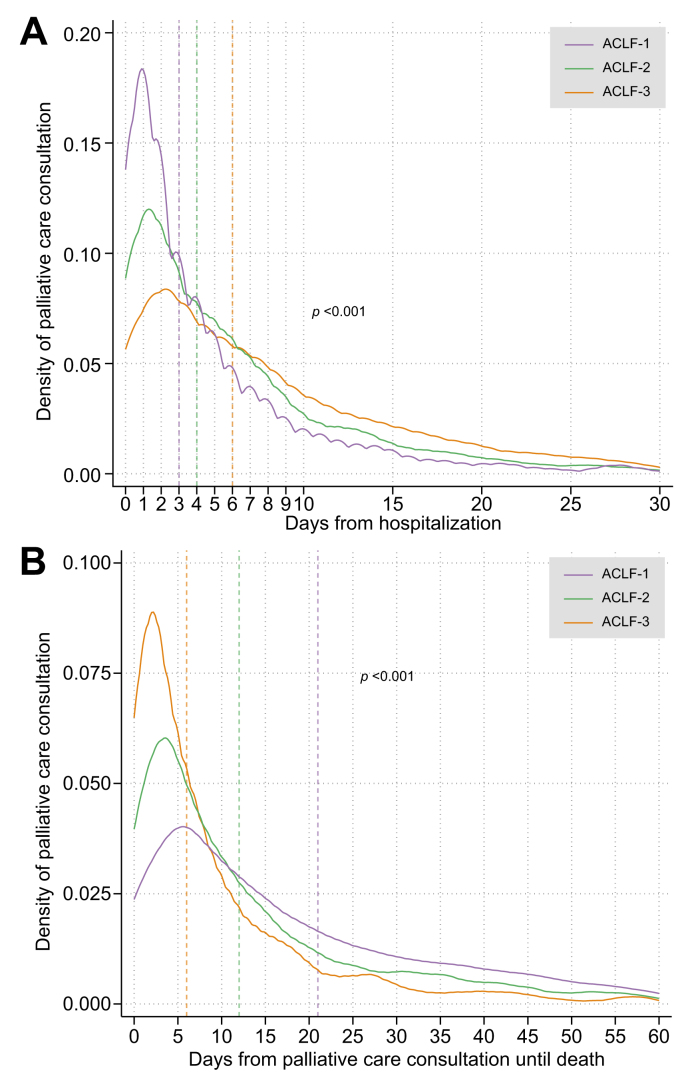
We identified 21,987 patients hospitalized with ACLF, of whom 30.5% received specialty palliative care consultation. Higher ACLF grade (ACLF-2 [odds ratio (OR) 1.82, 95% CI 1.67-1.99], ACLF-3 [OR 3.06, 95% CI 2.76-3.40]), prior specialty palliative care consultation (OR 2.62, 95% CI 2.36-2.91), and hepatocellular carcinoma (OR 2.10, 95% CI 1.89-2.33) were associated with consultation. Consultation occurred latest and closest to the time of death for patients with ACLF-3 compared to ACLF-1 and ACLF-2. Significant facility-level variation in consultation persisted among patients with ACLF-3, despite adjusting for multiple patient and facility factors.
In this large cohort of hospitalized patients with ACLF, specialty palliative care consultation was rare, more common in patients with higher grade ACLF, and tended to occur closer to the time of death for the sickest patients. Greater attention should be placed on earlier integration of palliative care during acute hospitalizations in patients with ACLF.
Though palliative care consultation is recommended for patients with acute-on-chronic liver failure, there is no data demonstrating how often this occurs during hospitalizations, on a population level. We found that consultation occurs in only 30.5% of patients and occurs later for patients with grade 3 acute-on-chronic liver failure. Our data should provoke clinicians to urgently consider quality improvement efforts to integrate palliative care into the management of these seriously ill patients.
姑息治疗原则应纳入影响肝脏的严重疾病(如慢加急性肝衰竭,ACLF)的管理中,这一观点越来越被接受。然而,ACLF患者中专科姑息治疗会诊的发生率、模式及预测因素尚未得到充分描述。
我们使用VOCAL队列对2008年1月1日至2018年12月31日期间因ACLF住院的患者进行了一项回顾性队列研究。对患者随访至2021年6月。我们使用混合效应回归分析来确定与姑息治疗会诊相关的重要患者和机构因素。我们研究了会诊时间、ACLF特征的影响以及机构层面差异对姑息治疗会诊接受情况的影响。
我们确定了21987例因ACLF住院的患者,其中30.5%接受了专科姑息治疗会诊。较高的ACLF分级(ACLF-2 [比值比(OR)1.82,95%置信区间1.67-1.99],ACLF-3 [OR 3.06,95%置信区间2.76-3.40])、既往专科姑息治疗会诊(OR 2.62,95%置信区间2.36-2.91)以及肝细胞癌(OR 2.10,95%置信区间1.89-2.33)与会诊相关。与ACLF-1和ACLF-2患者相比,ACLF-3患者的会诊发生时间最晚且最接近死亡时间。尽管对多个患者和机构因素进行了调整,但ACLF-3患者之间在会诊方面仍存在显著的机构层面差异。
在这一大型ACLF住院患者队列中,专科姑息治疗会诊很少见,在ACLF分级较高的患者中更常见,并且病情最严重的患者往往在更接近死亡时才进行会诊。对于ACLF患者,在急性住院期间应更加重视早期整合姑息治疗。
尽管推荐对慢加急性肝衰竭患者进行姑息治疗会诊,但在人群层面上,尚无数据表明住院期间这种情况发生的频率。我们发现只有30.5%的患者进行了会诊,且3级慢加急性肝衰竭患者的会诊时间较晚。我们的数据应促使临床医生迫切考虑采取质量改进措施,将姑息治疗纳入这些重症患者的管理中。