Shekhtman Louis, Cotler Scott J, Degasperi Elisabetta, Anolli Maria Paola, Uceda Renteria Sara Colonia, Sambarino Dana, Borghi Marta, Perbellini Riccardo, Facchetti Floriana, Ceriotti Ferruccio, Lampertico Pietro, Dahari Harel
The Program for Experimental & Theoretical Modeling, Division of Hepatology, Department of Medicine, Stritch School of Medicine, Loyola University Chicago, Maywood, IL, USA.
Department of Information Science, Bar-Ilan University, Ramat Gan, Israel.
JHEP Rep. 2023 Nov 15;6(2):100966. doi: 10.1016/j.jhepr.2023.100966. eCollection 2024 Feb.
BACKGROUND & AIMS: Bulevirtide (BLV) was approved for the treatment of compensated chronic hepatitis D virus (HDV) infection in Europe in 2020. However, research into the effects of the entry inhibitor BLV on HDV-host dynamics is in its infancy.
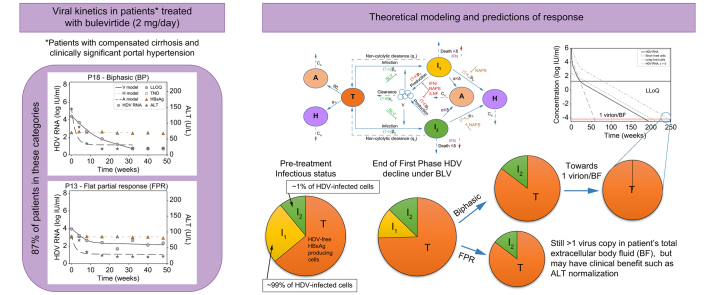
Eighteen patients with HDV under nucleos(t)ide analogue treatment for hepatitis B, with compensated cirrhosis and clinically significant portal hypertension, received BLV 2 mg/day. HDV RNA, alanine aminotransferase (ALT), and hepatitis B surface antigen (HBsAg) were measured at baseline, weeks 4, 8 and every 8 weeks thereafter. A mathematical model was developed to account for HDV, HBsAg and ALT dynamics during BLV treatment.
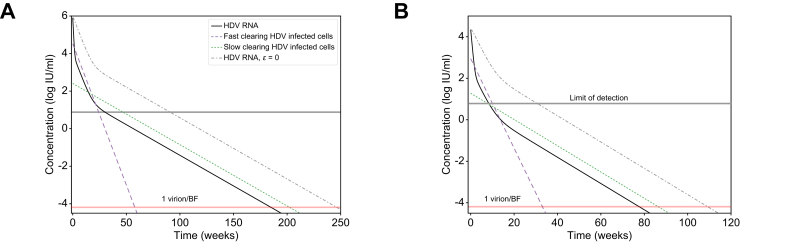
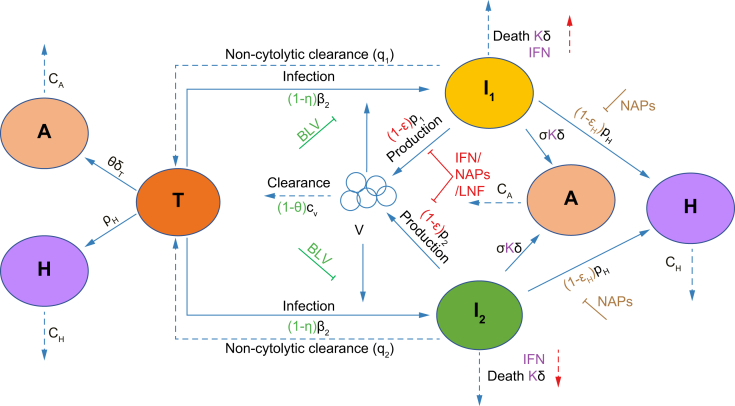
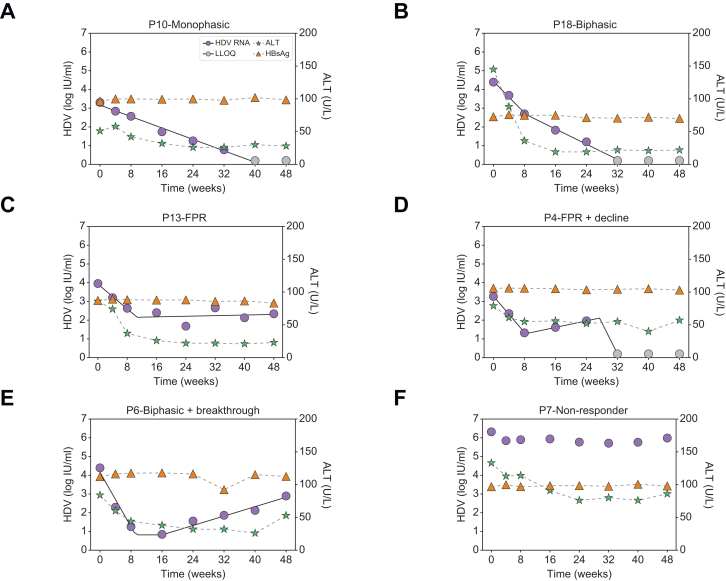
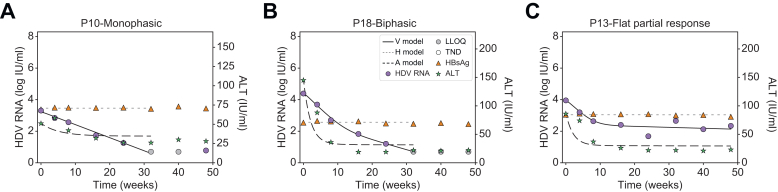
Median baseline HDV RNA, HBsAg, and ALT were 4.9 log IU/ml [IQR: 4.4-5.8], 3.7 log IU/ml [IQR: 3.4-3.9] and 106 U/L [IQR: 81-142], respectively. During therapy, patients fit into four main HDV kinetic patterns: monophasic (n = 2), biphasic (n = 10), flat-partial response (n = 4), and non-responder (n = 2). ALT normalization was achieved in 14 (78%) patients at a median of 8 weeks (range: 4-16). HBsAg remained at pre-treatment levels. Assuming that BLV completely (∼100%) blocks HDV entry, modeling indicated that two HDV-infected cell populations exist: fast HDV clearing (median t = 13 days) and slow HDV clearing (median t = 44 days), where the slow HDV-clearing population consisted of ∼1% of total HDV-infected cells, which could explain why most patients exhibited a non-monophasic pattern of HDV decline. Moreover, modeling explained ALT normalization without a change in HBsAg based on a non-cytolytic loss of HDV from infected cells, resulting in HDV-free HBsAg-producing cells that release ALT upon death at a substantially lower rate compared to HDV-infected cells.
The entry inhibitor BLV provides a unique opportunity to understand HDV, HBsAg, ALT, and host dynamics.
Mathematical modeling of hepatitis D virus (HDV) treatment with the entry inhibitor bulevirtide (BLV) provides a novel window into the dynamics of HDV RNA and alanine aminotransferase. Kinetic data from patients treated with BLV monotherapy can be explained by hepatocyte populations with different basal HDV clearance rates and non-cytolytic clearance of infected cells. While further studies are needed to test and refine the kinetic characterization described here, this study provides a new perspective on viral dynamics, which could inform evolving treatment strategies for HDV.
2020年,布立伏定(BLV)在欧洲被批准用于治疗代偿期慢性丁型肝炎病毒(HDV)感染。然而,关于进入抑制剂BLV对HDV-宿主动态影响的研究尚处于起步阶段。
18例接受核苷(酸)类似物治疗乙型肝炎、患有代偿期肝硬化且有临床显著门静脉高压的HDV患者,接受每日2毫克的BLV治疗。在基线、第4周、第8周以及此后每8周测量HDV RNA、丙氨酸氨基转移酶(ALT)和乙型肝炎表面抗原(HBsAg)。建立了一个数学模型来解释BLV治疗期间HDV、HBsAg和ALT的动态变化。
基线时HDV RNA、HBsAg和ALT的中位数分别为4.9 log IU/ml[四分位间距(IQR):4.4 - 5.8]、3.7 log IU/ml[IQR:3.4 - 3.9]和106 U/L[IQR:81 - 142]。在治疗期间,患者可分为四种主要的HDV动力学模式:单相(n = 2)、双相(n = 10)、平缓部分反应(n = 4)和无反应者(n = 2)。14例(78%)患者在中位数8周(范围:4 - 16周)时实现ALT正常化。HBsAg维持在治疗前水平。假设BLV完全(约100%)阻断HDV进入,模型表明存在两个HDV感染细胞群体:快速清除HDV(中位数t = 13天)和缓慢清除HDV(中位数t = 44天),其中缓慢清除HDV的群体约占HDV感染细胞总数的1%,这可以解释为什么大多数患者表现出HDV下降的非单相模式。此外,该模型解释了在HBsAg无变化的情况下ALT正常化,这是基于感染细胞中HDV的非细胞溶解性损失,导致产生无HDV的HBsAg细胞,这些细胞死亡时释放ALT的速率远低于HDV感染细胞。
进入抑制剂BLV为了解HDV、HBsAg、ALT和宿主动态提供了独特的机会。
用进入抑制剂布立伏定(BLV)治疗丁型肝炎病毒(HDV)的数学模型为HDV RNA和丙氨酸氨基转移酶的动态变化提供了一个新窗口。接受BLV单药治疗患者的动力学数据可以通过具有不同基础HDV清除率的肝细胞群体和感染细胞的非细胞溶解性清除来解释。虽然需要进一步研究来测试和完善此处描述的动力学特征,但本研究为病毒动态变化提供了新的视角,可为HDV不断发展的治疗策略提供参考。