El Messaoudi Selma, Brichler Ségolène, Fougerou-Leurent Claire, Gordien Emmanuel, Gerber Athenaïs, Kortebi Amal, Lagadic Garance, Subic-Levrero Miroslava, Metivier Sophie, Pol Stanislas, Minello Anne, Ratziu Vlad, Leroy Vincent, Mathurin Philippe, Alric Laurent, Coulibaly Fatoumata, Pawlotsky Jean-Michel, Zoulim Fabien, de Lédinghen Victor, Guedj Jérémie
Université Paris Cité, IAME, Inserm, Paris, France.
National Reference Center for Viral Hepatitis B, C, and D, Department of Clinical Microbiology, Hôpital Avicenne AP-HP, Université Sorbonne Paris Nord, Bobigny, INSERM U955, Créteil, France.
JHEP Rep. 2024 Mar 24;6(8):101070. doi: 10.1016/j.jhepr.2024.101070. eCollection 2024 Aug.
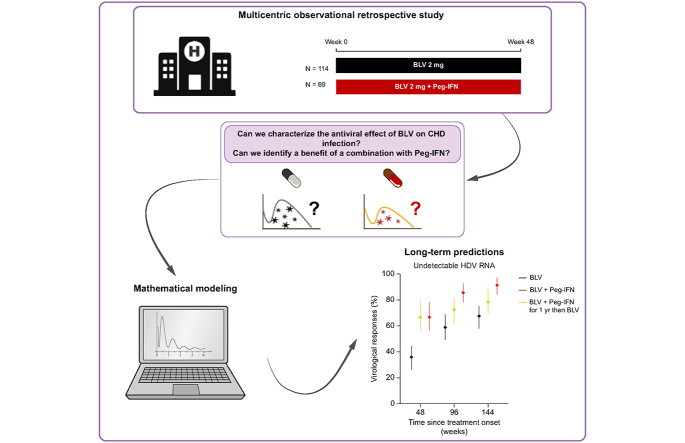
BACKGROUND & AIMS: Bulevirtide is a first-in-class entry inhibitor antiviral treatment for chronic hepatitis D. The viral kinetics during bulevirtide therapy and the effect of combining bulevirtide with pegylated-interferon (Peg-IFN) are unknown.
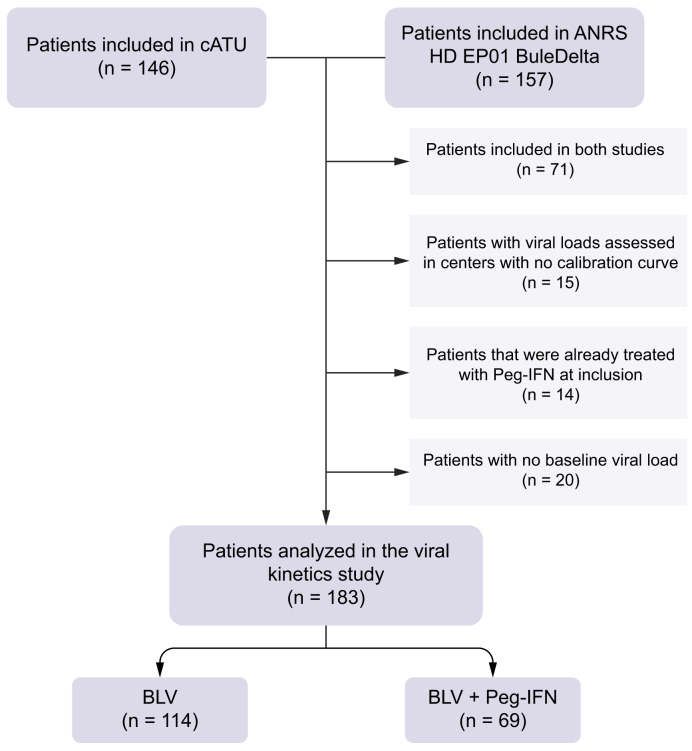
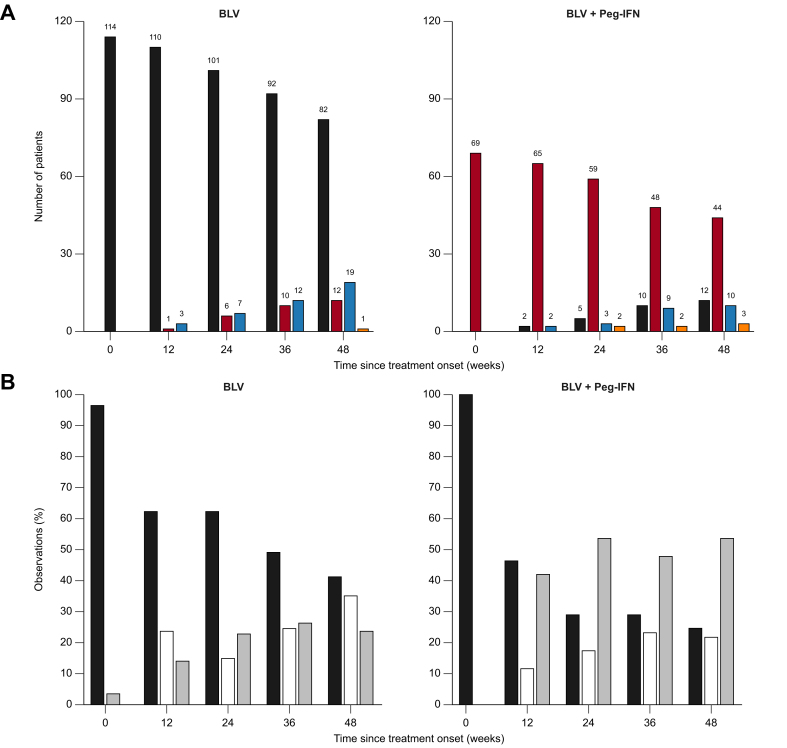
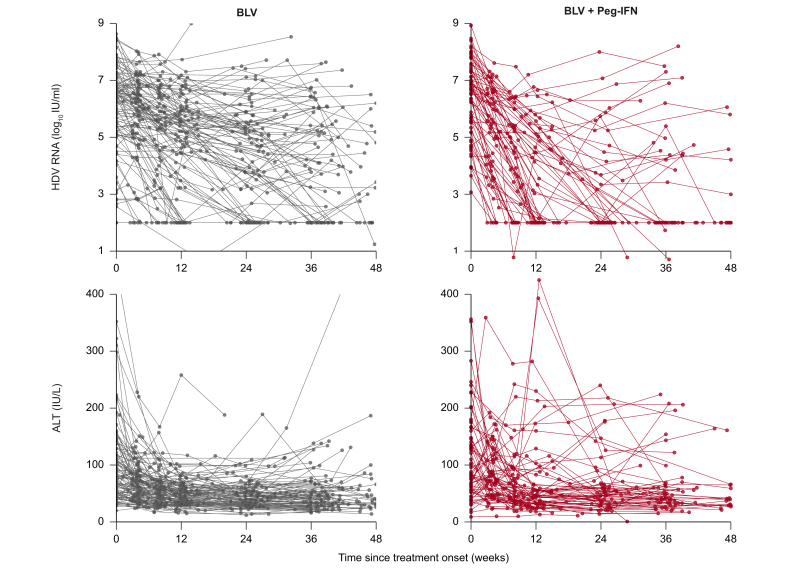
We used mathematical modelling to analyze the viral kinetics in two French observational cohorts of 183 patients receiving bulevirtide with or without Peg-IFN for 48 weeks.
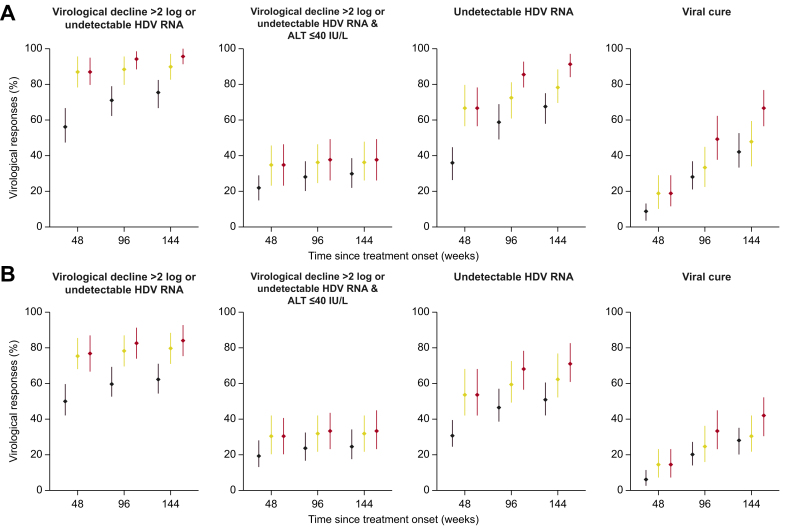
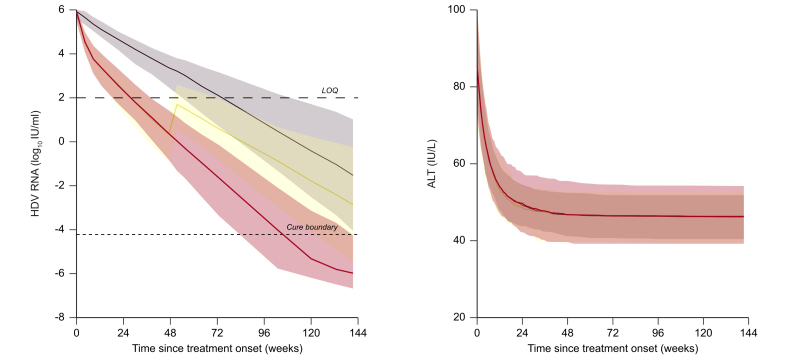
The efficacy of bulevirtide in blocking cell infection was estimated to 90.3%, whereas Peg-IFN blocked viral production with an efficacy of 92.4%, albeit with large inter-individual variabilities. The addition of Peg-IFN to bulevirtide was associated with a more rapid virological decline, with a rate of virological response (>2 log of decline or undetectability) at week 48 of 86.9% (95% prediction interval [PI] = [79.7-95.0]), compared with 56.1% (95% PI = [46.4-66.7]) with bulevirtide only. The model was also used to predict the probability to achieve a cure of viral infection, with a rate of 8.8% (95% PI = [3.5-13.2]) with bulevirtide compared with 18.8% (95% PI = [11.6-29.0]) with bulevirtide + Peg-IFN. Mathematical modelling suggests that after 144 weeks of treatment, the rates of viral cure could be 42.1% (95% PI = [33.3-52.6]) with bulevirtide and 66.7% (95% PI = [56.5-76.8]) with bulevirtide + Peg-IFN.
In this analysis of real-world data, Peg-IFN strongly enhanced the kinetics of viral decline in patients treated with bulevirtide. Randomized clinical trials are warranted to assess the virological and clinical benefit of this combination, and to identify predictors of poor response to treatment.
Bulevirtide has been approved for chronic HDV infection by regulatory agencies in Europe based on its good safety profile and rapid virological response after treatment initiation, but the optimal duration of treatment and the chance to achieve a sustained virological response remain unknown. The results presented in this study have a high impact for clinicians and investigators as they provide important knowledge on the long-term virological benefits of a combination of Peg-IFN and bulevirtide in patients with CHD. Clinical trials are now warranted to confirm those predictions.
布列韦替德是用于慢性丁型肝炎的首个一流的进入抑制剂抗病毒疗法。布列韦替德治疗期间的病毒动力学以及布列韦替德与聚乙二醇干扰素(Peg-IFN)联合使用的效果尚不清楚。
我们使用数学建模分析了两个法国观察性队列中183例接受布列韦替德治疗(有或无Peg-IFN)48周的患者的病毒动力学。
布列韦替德阻断细胞感染的疗效估计为90.3%,而Peg-IFN阻断病毒产生的疗效为92.4%,尽管个体间差异较大。在布列韦替德基础上加用Peg-IFN与病毒学下降更快相关,在第48周时病毒学应答率(下降>2 log或检测不到)为86.9%(95%预测区间[PI]=[79.7-95.0]),而仅用布列韦替德时为56.1%(95% PI=[46.4-66.7])。该模型还用于预测病毒感染治愈的概率,布列韦替德治疗的治愈率为8.8%(95% PI=[3.5-13.2]),而布列韦替德+Peg-IFN治疗的治愈率为18.8%(95% PI=[11.6-29.0])。数学建模表明,治疗144周后,布列韦替德治疗的病毒治愈率可能为42.1%(95% PI=[33.3-52.6]),布列韦替德+Peg-IFN治疗的病毒治愈率可能为66.7%(95% PI=[56.5-76.8])。
在这项对真实世界数据的分析中,Peg-IFN显著增强了接受布列韦替德治疗患者的病毒下降动力学。有必要进行随机临床试验以评估这种联合治疗的病毒学和临床益处,并确定治疗反应不佳的预测因素。
基于其良好的安全性和治疗开始后的快速病毒学应答,布列韦替德已被欧洲监管机构批准用于慢性丁型肝炎病毒感染,但最佳治疗持续时间和实现持续病毒学应答的机会仍不清楚。本研究结果对临床医生和研究人员具有重大影响,因为它们提供了关于Peg-IFN与布列韦替德联合治疗对慢性丁型肝炎患者长期病毒学益处的重要知识。现在有必要进行临床试验以证实这些预测。