Institute of Pathology, Heidelberg University Hospital, Heidelberg, Germany.
Translational Lung Research Center (TLRC) Heidelberg, Member of the German Center for Lung Research (DZL), Heidelberg, Germany.
J Pathol Clin Res. 2024 Mar;10(2):e354. doi: 10.1002/cjp2.354.
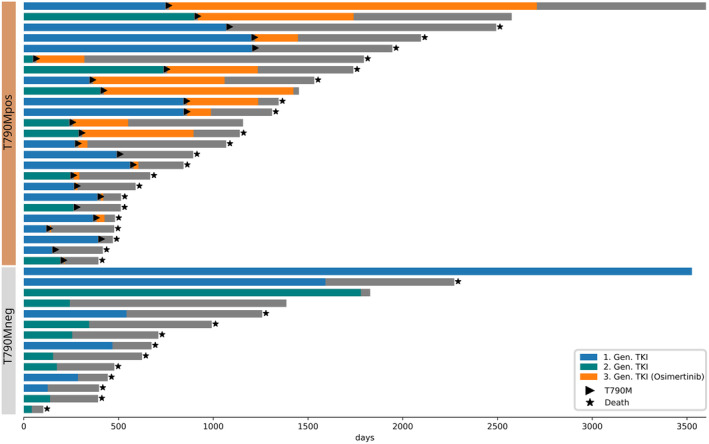
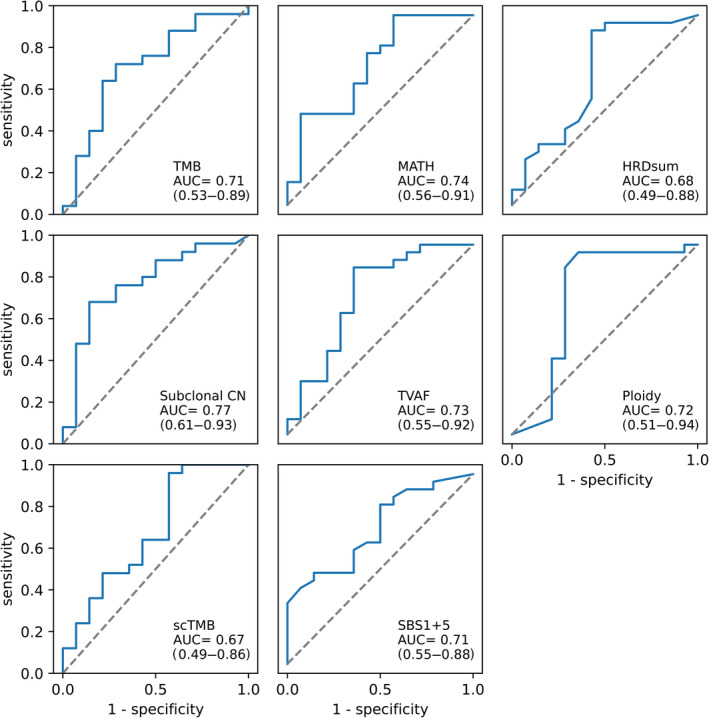
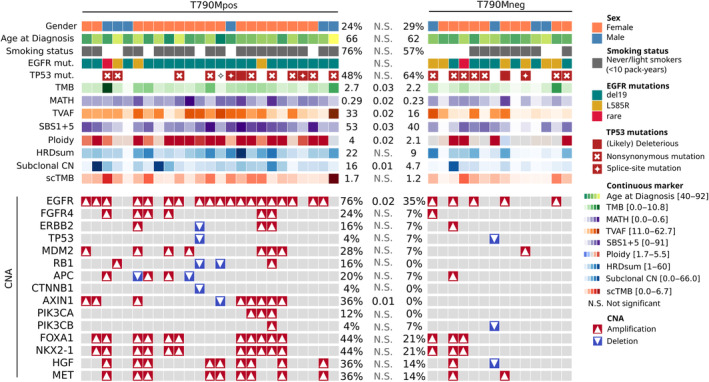
This study analyzed whether extended molecular profiling can predict the development of epidermal growth factor receptor (EGFR) gene T790M mutation, which is the most frequent resistance alteration in non-small cell lung cancer (NSCLC) after treatment with the first-/second-generation (1G/2G) EGFR inhibitors (tyrosine kinase inhibitors [TKIs]), but only weakly associated with clinical characteristics. Whole exome sequencing (WES) was performed on pretreatment tumor tissue with matched normal samples from NSCLC patients with (n = 25, detected in tissue or blood rebiopsies) or without (n = 14, negative tissue rebiopsies only) subsequent EGFR p.T790M mutation after treatment with 1G/2G EGFR TKI. Several complex genetic biomarkers were assessed using bioinformatic methods. After treatment with first-line afatinib (44%) or erlotinib/gefitinib (56%), median progression-free survival and overall survival were 12.1 and 33.7 months, respectively. Clinical and tumor genetic characteristics, including age (median, 66 years), sex (74% female), smoking (69% never/light smokers), EGFR mutation type (72% exon 19 deletions), and TP53 mutations (41%) were not significantly associated with T790M mutation (p > 0.05). By contrast, complex biomarkers including tumor mutational burden, the clock-like mutation signature SBS1 + 5, tumor ploidy, and markers of subclonality including mutant-allele tumor heterogeneity, subclonal copy number changes, and median tumor-adjusted variant allele frequency were significantly higher at baseline in tumors with subsequent T790M mutation (all p < 0.05). Each marker alone could predict subsequent development of T790M with an area under the curve (AUC) of 0.72-0.77, but the small number of cases did not allow confirmation of better performance for biomarker combinations in leave-one-out cross-validated logistic regression (AUC 0.69, 95% confidence interval: 0.50-0.87). Extended molecular profiling with WES at initial diagnosis reveals several complex biomarkers associated with subsequent development of T790M resistance mutation in NSCLC patients receiving first-/second-generation TKIs as the first-line therapy. Larger prospective studies will be necessary to define a forecasting model.
本研究分析了扩展分子谱是否可以预测表皮生长因子受体(EGFR)基因 T790M 突变的发展,这是接受第一代/第二代(1G/2G)EGFR 抑制剂(酪氨酸激酶抑制剂[TKI])治疗后非小细胞肺癌(NSCLC)最常见的耐药改变,但与临床特征的相关性较弱。对接受 1G/2G EGFR TKI 一线治疗后出现 EGFR p.T790M 突变的 NSCLC 患者的预处理肿瘤组织和匹配的正常样本(n=25,在组织或血液再活检中检测到)或无(n=14,仅组织再活检阴性)进行全外显子组测序(WES)。使用生物信息学方法评估了几种复杂的遗传生物标志物。接受一线阿法替尼(44%)或厄洛替尼/吉非替尼(56%)治疗后,中位无进展生存期和总生存期分别为 12.1 个月和 33.7 个月。临床和肿瘤遗传特征,包括年龄(中位数,66 岁)、性别(74%为女性)、吸烟史(69%为从不/轻度吸烟者)、EGFR 突变类型(72%为外显子 19 缺失)和 TP53 突变(41%)与 T790M 突变(p>0.05)无显著相关性。相比之下,在随后发生 T790M 突变的肿瘤中,基线时肿瘤突变负担、时钟样突变特征 SBS1+5、肿瘤倍性以及包括突变等位基因肿瘤异质性、亚克隆拷贝数变化和中位肿瘤调整变异等位基因频率在内的亚克隆标志物等复杂标志物显著更高(均 p<0.05)。每个标志物单独预测 T790M 突变的曲线下面积(AUC)为 0.72-0.77,但由于病例数较少,无法在留一法交叉验证逻辑回归中确认标志物组合的性能更好(AUC 0.69,95%置信区间:0.50-0.87)。在接受第一代/第二代 TKI 作为一线治疗的 NSCLC 患者中,在初始诊断时进行 WES 扩展分子谱分析可以揭示与随后发生 T790M 耐药突变相关的几种复杂生物标志物。需要进行更大规模的前瞻性研究来确定预测模型。