Bhatia Harpreet S, Trainor Patrick, Carlisle Samantha, Tsai Michael Y, Criqui Michael H, DeFilippis Andrew, Tsimikas Sotirios
Division of Cardiovascular Medicine, Department of Medicine University of California, San Diego La Jolla CA.
Department of Chemistry and Biochemistry New Mexico State University Las Cruces NM.
J Am Heart Assoc. 2024 Feb 6;13(3):e033562. doi: 10.1161/JAHA.123.033562. Epub 2024 Jan 31.
Effective therapies for reducing cardiovascular disease (CVD) risk in people with elevated lipoprotein(a) are lacking, especially for primary prevention. Because of the potential association of lipoprotein(a) with thrombosis, we evaluated the relationship between aspirin use and CVD events in people with elevated lipoprotein(a).
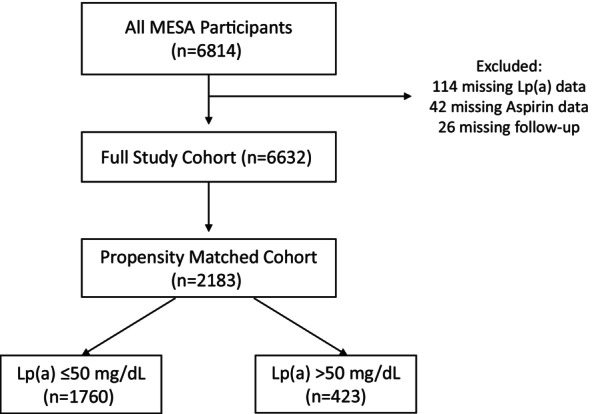
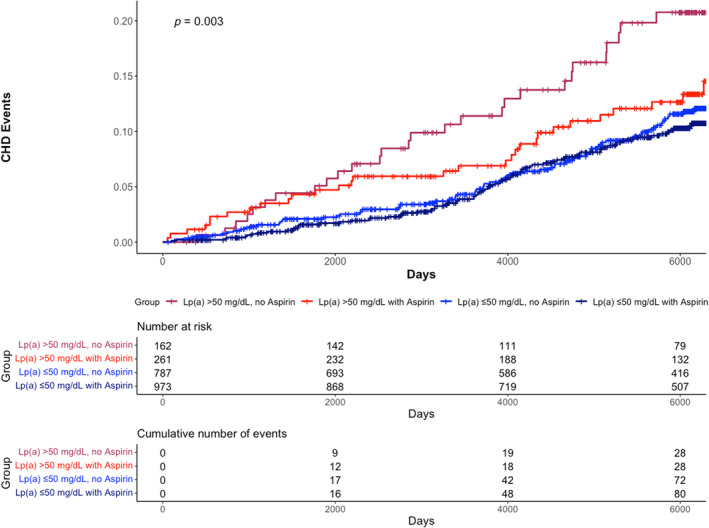
We used data from the MESA (Multi-Ethnic Study of Atherosclerosis), a prospective cohort study of individuals free of baseline cardiovascular disease. Due to potential confounding by indication, we matched aspirin users to nonusers using a propensity score based on CVD risk factors. We then evaluated the association between aspirin use and coronary heart disease (CHD) events (CHD death, nonfatal myocardial infarction) stratified by baseline lipoprotein(a) level (threshold of 50 mg/dL) using Cox proportional hazards models with adjustment for CVD risk factors. After propensity matching, the study cohort included 2183 participants, including 1234 (57%) with baseline aspirin use and 423 (19%) with lipoprotein(a) >50 mg/dL. Participants with lipoprotein(a) >50 mg/dL had a higher burden of CVD risk factors, more frequent aspirin use (61.7% versus 55.3%, =0.02), and higher rate of incident CHD events (13.7% versus 8.9%, <0.01). Aspirin was associated with a significant reduction in CHD events among those with elevated lipoprotein(a) (hazard ratio, 0.54 [95% CI, 0.32-0.94]; =0.03). Those with lipoprotein(a) >50 mg/dL and aspirin use had similar CHD risk as those with lipoprotein(a) ≤50 mg/dL regardless of aspirin use.
Aspirin use was associated with a significantly lower risk for CHD events in participants with lipoprotein(a) >50 mg/dL without baseline CVD. The results of this observational propensity-matched study require confirmation in studies with randomization of aspirin use.
缺乏有效降低脂蛋白(a)升高人群心血管疾病(CVD)风险的疗法,尤其是一级预防方面。鉴于脂蛋白(a)与血栓形成的潜在关联,我们评估了阿司匹林使用与脂蛋白(a)升高人群CVD事件之间的关系。
我们使用了动脉粥样硬化多族裔研究(MESA)的数据,这是一项针对无基线心血管疾病个体的前瞻性队列研究。由于存在指征性潜在混杂因素,我们根据CVD危险因素使用倾向评分将阿司匹林使用者与非使用者进行匹配。然后,我们使用Cox比例风险模型,在对CVD危险因素进行调整的情况下,评估阿司匹林使用与按基线脂蛋白(a)水平(阈值为50mg/dL)分层的冠心病(CHD)事件(CHD死亡、非致命性心肌梗死)之间的关联。倾向匹配后,研究队列包括2183名参与者,其中1234名(57%)基线使用阿司匹林,423名(19%)脂蛋白(a)>50mg/dL。脂蛋白(a)>50mg/dL的参与者CVD危险因素负担更高,阿司匹林使用更频繁(61.7%对55.3%,P=0.02),CHD事件发生率更高(13.7%对8.9%,P<0.01)。阿司匹林与脂蛋白(a)升高人群的CHD事件显著减少相关(风险比,0.54[95%CI,0.32 - 0.94];P=0.03)。脂蛋白(a)>50mg/dL且使用阿司匹林的人群与脂蛋白(a)≤50mg/dL的人群无论是否使用阿司匹林,CHD风险相似。
在无基线CVD且脂蛋白(a)>50mg/dL的参与者中,使用阿司匹林与CHD事件风险显著降低相关。这项观察性倾向匹配研究的结果需要在阿司匹林使用随机化的研究中得到证实。