Department of Clinical Neurosciences, Neurosurgery Service and Gamma Knife Center, Lausanne University Hospital (CHUV), Rue du Bugnon 44-46, BH-08, CH-1011, Lausanne, Switzerland.
Faculty of Biology and Medicine (FBM), University of Lausanne (UNIL), Lausanne, Switzerland.
Neurosurg Rev. 2024 Jan 31;47(1):73. doi: 10.1007/s10143-024-02296-1.
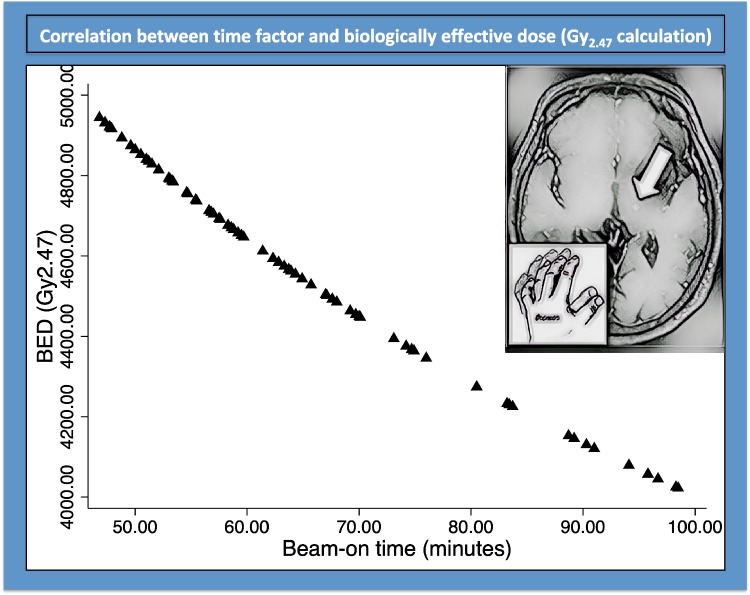
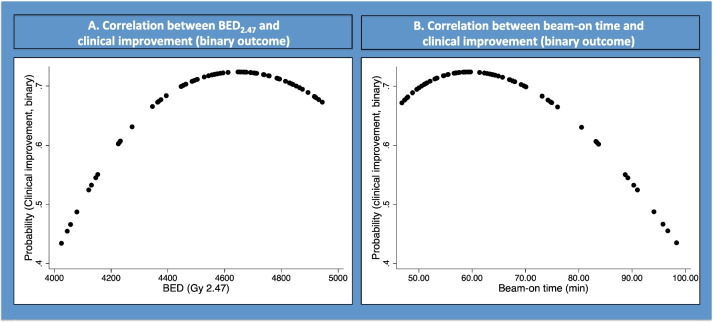
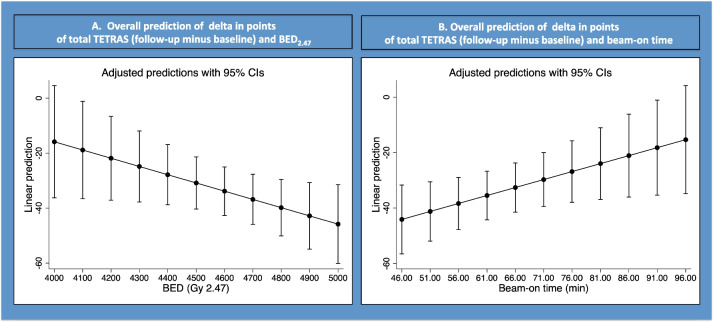
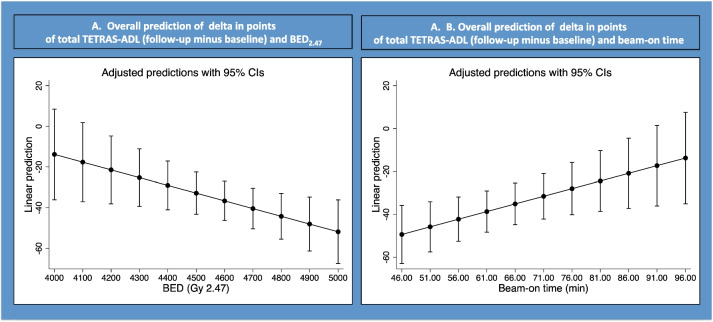
Stereotactic radiosurgery (SRS) is one of the surgical alternatives for drug-resistant essential tremor (ET). Here, we aimed at evaluating whether biologically effective dose (BED) is relevant for tremor improvement after stereotactic radiosurgical thalamotomy in a population of patients treated with one (unplugged) isocenter and a uniform dose of 130 Gy. This is a retrospective longitudinal single center study. Seventy-eight consecutive patients were clinically analyzed. Mean age was 69.1 years (median 71, range 36-88). Mean follow-up period was 14 months (median 12, 3-36). Tremor improvement was assessed at 12 months after SRS using the ET rating assessment scale (TETRAS, continuous outcome) and binary (binary outcome). BED was defined for an alpha/beta of 2.47, based upon previous studies considering such a value for the normal brain. Mean BED was 4573.1 Gy (median 4612, 4022.1-4944.7). Mean beam-on time was 64.7 min (median 61.4; 46.8-98.5). There was a statically significant correlation between delta (follow-up minus baseline) in TETRAS (total) with BED (p = 0.04; beta coefficient - 0.029) and beam-on time (p = 0.03; beta coefficient 0.57) but also between TETRAS (ADL) with BED (p = 0.02; beta coefficient 0.038) and beam-on time (p = 0.01; beta coefficient 0.71). Fractional polynomial multivariate regression suggested that a BED > 4600 Gy and a beam-on time > 70 min did not further increase clinical efficacy (binary outcome). Adverse radiation events (ARE) were defined as larger MR signature on 1-year follow-up MRI and were present in 7 out of 78 (8.9%) cases, receiving a mean BED of 4650 Gy (median 4650, range 4466-4894). They were clinically relevant with transient hemiparesis in 5 (6.4%) patients, all with BED values higher than 4500 Gy. Tremor improvement was correlated with BED Gy after SRS for drug-resistant ET. An optimal BED value for tremor improvement was 4300-4500 Gy. ARE appeared for a BED of more than 4500 Gy. Such finding should be validated in larger cohorts.
立体定向放射外科(SRS)是治疗耐药性特发性震颤(ET)的手术选择之一。在这里,我们旨在评估在接受一个(未插入)等中心和 130Gy 均匀剂量治疗的患者群体中,生物有效剂量(BED)是否与立体定向放射外科丘脑切开术后震颤改善相关。这是一项回顾性纵向单中心研究。对 78 例连续患者进行了临床分析。平均年龄为 69.1 岁(中位数 71,范围 36-88)。平均随访时间为 14 个月(中位数 12,3-36)。SRS 后 12 个月使用 ET 评分评估量表(TETRAS,连续结果)和二进制(二进制结果)评估震颤改善。根据先前考虑到正常脑的 2.47 这种值的研究,定义了 BED 为 α/β=2.47。平均 BED 为 4573.1Gy(中位数 4612,4022.1-4944.7)。平均照射时间为 64.7 分钟(中位数 61.4;46.8-98.5)。TETRAS(总)的随访与基线之间的差值(δ)与 BED(p=0.04;β系数-0.029)和照射时间(p=0.03;β系数 0.57)之间存在统计学显著相关性,但 TETRAS(ADL)与 BED(p=0.02;β系数 0.038)和照射时间(p=0.01;β系数 0.71)之间也存在相关性。分数多项式多变量回归表明,BED>4600Gy 和照射时间>70 分钟不会进一步提高临床疗效(二进制结果)。放射性不良事件(ARE)定义为在 1 年随访 MRI 上出现更大的 MR 特征,78 例中有 7 例(8.9%)出现,接受平均 BED 为 4650Gy(中位数 4650,范围 4466-4894)。5 例(6.4%)患者出现临床相关的短暂偏瘫,所有患者的 BED 值均高于 4500Gy。SRS 治疗耐药性 ET 后,震颤改善与 BEDGy 相关。BED 改善震颤的最佳值为 4300-4500Gy。当 BED 大于 4500Gy 时,会出现 ARE。这一发现应在更大的队列中得到验证。