State Key Laboratory of Oncology in South China, Guangdong Key Laboratory of Nasopharyngeal Carcinoma Diagnosis and Therapy, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, China.
Department of Radiology, Sun Yat-Sen University Cancer Center, Guangzhou, China.
Eur Radiol. 2024 Sep;34(9):6047-6059. doi: 10.1007/s00330-024-10598-7. Epub 2024 Feb 3.
The prognostic stratification for oral tongue squamous cell carcinoma (OTSCC) is heavily based on postoperative pathological depth of invasion (pDOI). This study aims to propose a preoperative MR T-staging system based on tumor size for non-pT4 OTSCC.
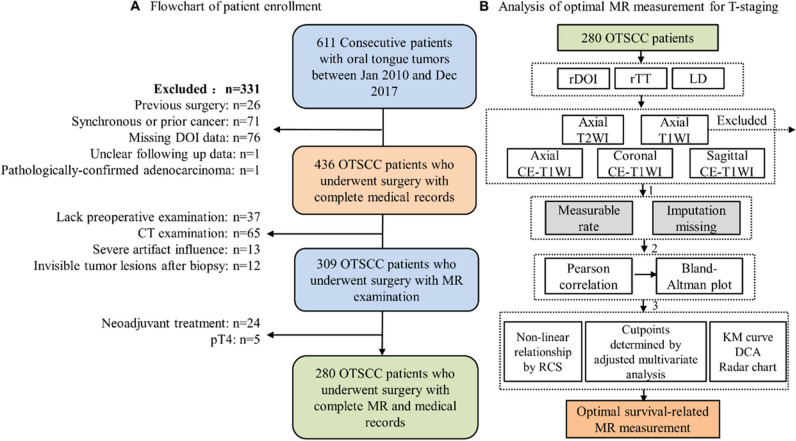
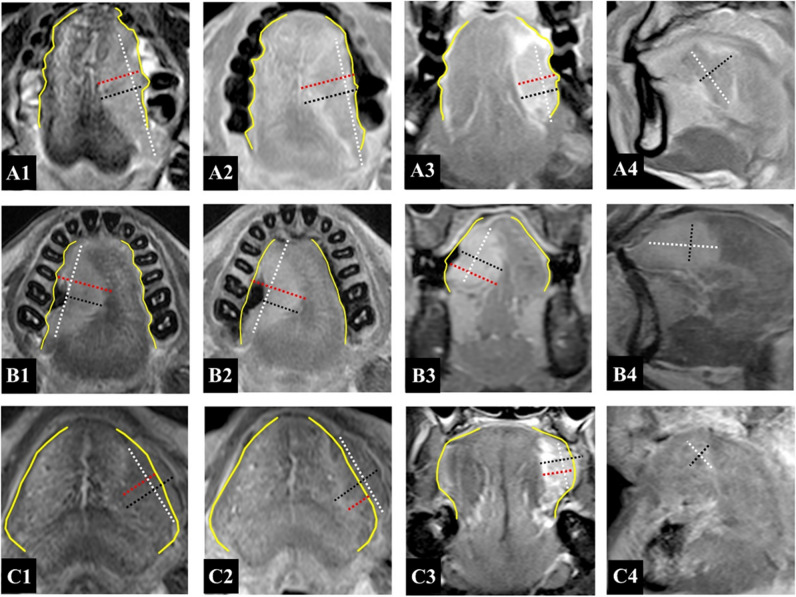
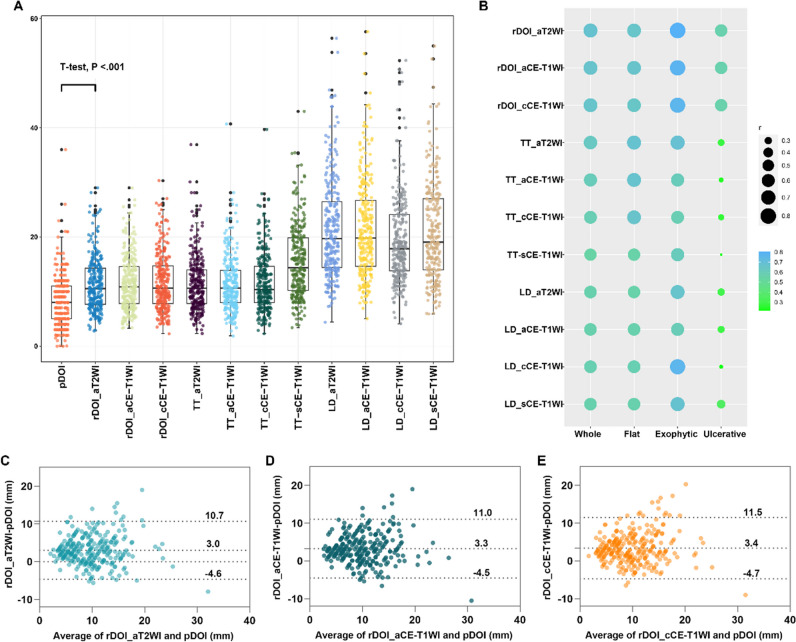
Retrospectively, 280 patients with biopsy-confirmed, non-metastatic, pT1-3 OTSCC, treated between January 2010 and December 2017, were evaluated. Multiple MR sequences, including axial T2-weighted imaging (WI), unenhanced T1WI, and axial, fat-suppressed coronal, and sagittal contrast-enhanced (CE) T1WI, were utilized to measure radiological depth of invasion (rDOI), tumor thickness, and largest diameter. Intra-class correlation (ICC) and univariate and multivariate analyses were used to evaluate measurement reproducibility, and factors' significance, respectively. Cutoff values were established using an exhaustive method.
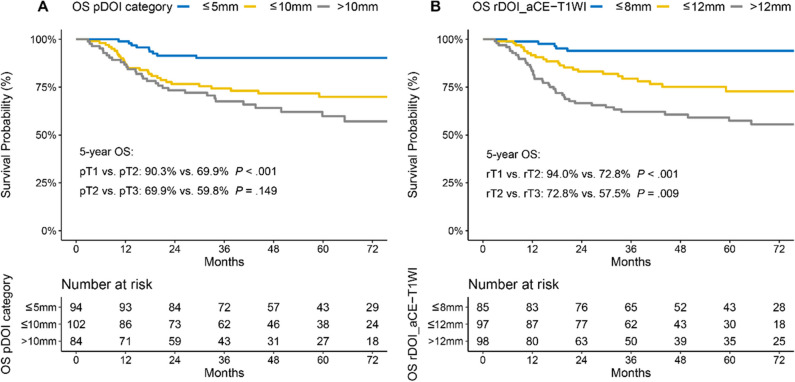
Intra-observer (ICC = 0.81-0.94) and inter-observer (ICC = 0.79-0.90) reliability were excellent for rDOI measurements, and all measurements were significantly associated with overall survival (OS) (all p < .001). Measuring the rDOI on axial CE-T1WI with cutoffs of 8 mm and 12 mm yielded an optimal MR T-staging system for rT1-3 disease (5-year OS of rT1 vs rT2 vs rT3: 94.0% vs 72.8% vs 57.5%). Using multivariate analyses, the proposed T-staging exhibited increasingly worse OS (hazard ratio of rT2 and rT3 versus rT1, 3.56 [1.35-9.6], p = .011; 4.33 [1.59-11.74], p = .004; respectively), which outperformed pathological T-staging based on nonoverlapping Kaplan-Meier curves and improved C-index (0.682 vs. 0.639, p < .001).
rDOI is a critical predictor of OTSCC mortality and facilitates preoperative prognostic stratification, which should be considered in future oral subsite MR T-staging.
Utilizing axial CE-T1WI, an MR T-staging system for non-pT4 OTSCC was developed by employing rDOI measurement with optimal thresholds of 8 mm and 12 mm, which is comparable with pathological staging and merits consideration in future preoperative oral subsite planning.
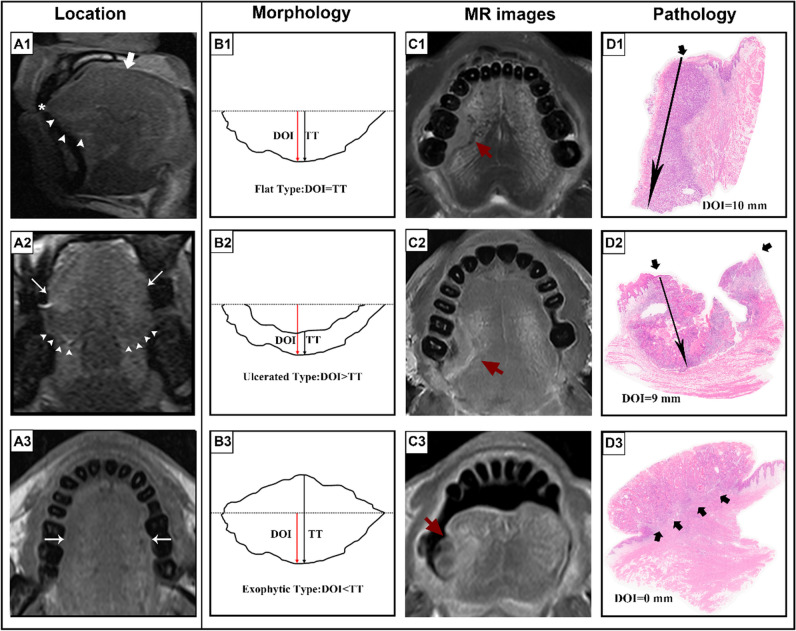
• Tumor morphology, measuring sequences, and observers could impact MR-derived measurements and compromise the consistency with histology. • MR-derived measurements, including radiological depth of invasion (rDOI), tumor thickness, and largest diameter, have a prognostic impact on OS (all p < .001). • rDOI with cutoffs of 8 mm and 12 mm on axial CE-T1WI is an optimal predictor of OS and could facilitate risk stratification in non-pT4 OTSCC disease.
口腔舌鳞状细胞癌(OTSCC)的预后分层主要基于术后病理浸润深度(pDOI)。本研究旨在提出一种基于肿瘤大小的非 pT4 OTSCC 的术前 MR T 分期系统。
回顾性分析了 2010 年 1 月至 2017 年 12 月期间经活检证实、无转移的 pT1-3 OTSCC 患者 280 例。使用包括轴位 T2 加权成像(WI)、未增强 T1WI 以及轴位、脂肪抑制冠状位和矢状位对比增强(CE)T1WI 在内的多种 MR 序列来测量放射学深度(rDOI)、肿瘤厚度和最大直径。采用组内相关系数(ICC)和单变量及多变量分析分别评估测量的可重复性和各因素的显著性。采用穷尽法建立临界值。
rDOI 测量的观察者内(ICC=0.81-0.94)和观察者间(ICC=0.79-0.90)可靠性均极好,所有测量均与总生存率(OS)显著相关(均 p<.001)。在轴向 CE-T1WI 上测量 rDOI,以 8mm 和 12mm 为截断值,可获得 rT1-3 疾病的最佳 MR T 分期系统(rT1 与 rT2 与 rT3 的 5 年 OS:94.0% vs 72.8% vs 57.5%)。采用多变量分析,所提出的 T 分期显示出越来越差的 OS(rT2 和 rT3 与 rT1 的危险比分别为 3.56[1.35-9.6],p=0.011;4.33[1.59-11.74],p=0.004),这优于基于非重叠 Kaplan-Meier 曲线和提高 C 指数的病理 T 分期(0.682 与 0.639,p<.001)。
rDOI 是 OTSCC 死亡率的关键预测因子,有助于术前预后分层,在未来的口腔亚部位 MR T 分期中应考虑这一因素。
利用轴向 CE-T1WI,通过使用最佳截断值为 8mm 和 12mm 的 rDOI 测量,建立了非 pT4 OTSCC 的 MR T 分期系统,该系统与病理分期相当,值得在未来的术前口腔亚部位规划中考虑。
肿瘤形态、测量序列和观察者可能会影响基于 MRI 的测量并影响与组织学的一致性。
包括放射学深度(rDOI)、肿瘤厚度和最大直径在内的 MRI 测量对 OS 有预后影响(均 p<.001)。
轴位 CE-T1WI 上 rDOI 截断值为 8mm 和 12mm 是 OS 的最佳预测因子,可促进非 pT4 OTSCC 疾病的风险分层。