O'Neal Hollis R, Sheybani Roya, Janz David R, Scoggins Robert, Jagneaux Tonya, Walker James E, Henning Daniel J, Rosenman Elizabeth, Mahler Simon A, Regunath Hariharan, Sampson Christopher S, Files D Clark, Fremont Richard D, Noto Michael J, Schneider Erica E, Shealey Wesley R, Berlinger Matthew S, Carver Thomas C, Walker Morgan K, Ledeboer Nathan A, Shah Ajay M, Tse Henry T K, DiCarlo Dino, Rice Todd W, Thomas Christopher B
Pulmonary and Critical Care, Louisiana State University Health Sciences Center, Baton Rouge, LA.
Pulmonary & Critical Care, Our Lady of the Lake Regional Medical Center, Baton Rouge, LA.
Crit Care Explor. 2024 Feb 7;6(2):e1026. doi: 10.1097/CCE.0000000000001026. eCollection 2024 Feb.
To assess the in vitro IntelliSep test, a microfluidic assay that quantifies the state of immune activation by evaluating the biophysical properties of leukocytes, as a rapid diagnostic for sepsis.
Prospective cohort study.
Five emergency departments (EDs) in Louisiana, Missouri, North Carolina, and Washington.
Adult patients presenting to the ED with signs (two of four Systemic Inflammatory Response Syndrome criteria, where one must be temperature or WBC count) or suspicion (provider-ordered culture) of infection.
All patients underwent testing with the IntelliSep using ethylene diamine tetraacetic acid-anticoagulated whole blood followed by retrospective adjudication for sepsis by sepsis-3 criteria by a blinded panel of physicians.
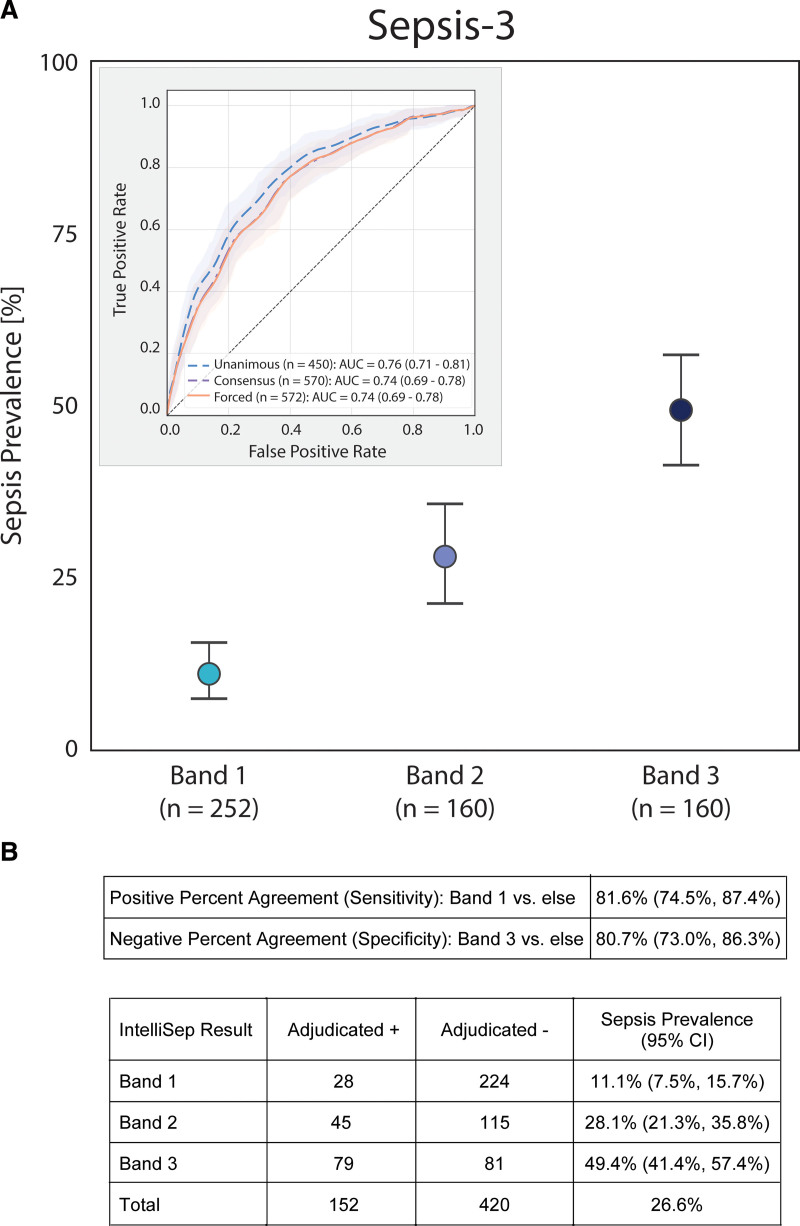
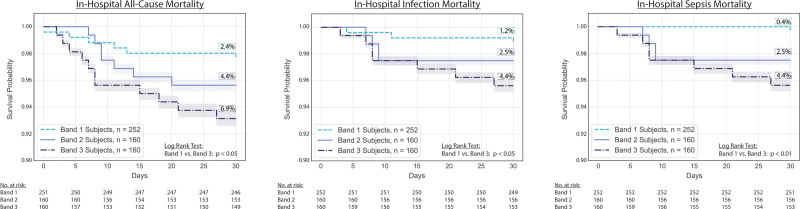
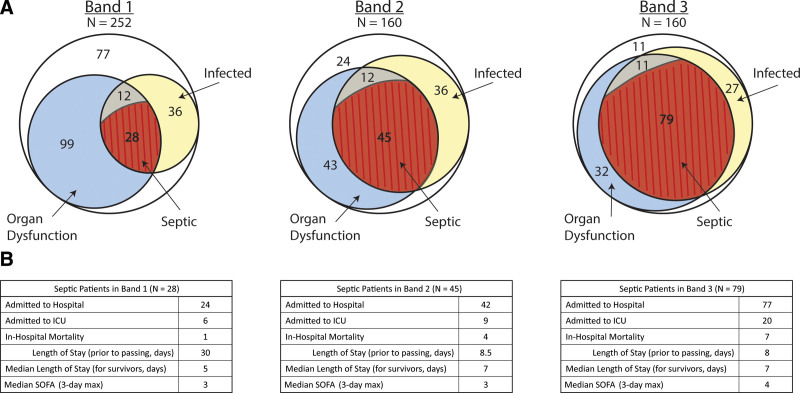
Of 599 patients enrolled, 572 patients were included in the final analysis. The result of the IntelliSep test is reported as the IntelliSep Index (ISI), ranging from 0.1 to 10.0, divided into three interpretation bands for the risk of sepsis: band 1 (low) to band 3 (high). The median turnaround time for ISI results was 7.2 minutes. The ISI resulted band 1 in 252 (44.1%), band 2 in 160 (28.0%), and band 3 in 160 (28.0%). Sepsis occurred in 26.6% (152 of 572 patients). Sepsis prevalence was 11.1% (95% CI, 7.5-15.7%) in band 1, 28.1% (95% CI, 21.3-35.8%) in band 2, and 49.4% (95% CI, 41.4-57.4%) in band 3. The Positive Percent Agreement of band 1 was 81.6% and the Negative Percent Agreement of band 3 was 80.7%, with an area under the receiver operating characteristic curve of 0.74. Compared with band 1, band 3 correlated with adverse clinical outcomes, including mortality, and resource utilization.
Increasing ISI interpretation band is associated with increasing probability of sepsis in patients presenting to the ED with suspected infection.
评估IntelliSep体外检测,这是一种通过评估白细胞的生物物理特性来量化免疫激活状态的微流控检测方法,作为脓毒症的快速诊断方法。
前瞻性队列研究。
路易斯安那州、密苏里州、北卡罗来纳州和华盛顿州的五个急诊科。
因感染体征(符合四项全身炎症反应综合征标准中的两项,其中一项必须是体温或白细胞计数)或疑似感染(医生医嘱进行培养)而到急诊科就诊的成年患者。
所有患者均使用乙二胺四乙酸抗凝全血进行IntelliSep检测,随后由一组盲法医生根据脓毒症-3标准对脓毒症进行回顾性判定。
在纳入的599例患者中,572例患者纳入最终分析。IntelliSep检测结果报告为IntelliSep指数(ISI),范围为0.1至10.0,分为脓毒症风险的三个解读区间:区间1(低)至区间3(高)。ISI结果的中位周转时间为7.2分钟。ISI结果处于区间1的有252例(44.1%),区间2的有160例(28.0%),区间3的有160例(28.0%)。脓毒症发生率为26.6%(572例患者中的152例)。区间1的脓毒症患病率为11.1%(95%CI,7.5-15.7%),区间2为28.1%(95%CI,21.3-35.8%),区间3为49.4%(95%CI,41.4-57.4%)。区间1的阳性百分比一致性为81.6%,区间3的阴性百分比一致性为80.7%,受试者工作特征曲线下面积为0.74。与区间1相比,区间3与不良临床结局相关,包括死亡率和资源利用情况。
对于到急诊科就诊且疑似感染的患者,ISI解读区间增加与脓毒症发生概率增加相关。