Mulinge Martin M, Kibui Nancy K, Kimani Humphrey, Wainaina Joseph, Bwana Priska, Omondi Martin, Wafula Kevin, Wamalwa Dalton C, Omondi Evans O, Nduati Ruth W, Mwau Matilu
Department of Biochemistry, University of Nairobi, Nairobi, Kenya.
Centre for Infectious and Parasitic Diseases Control Research, Kenya Medical Research Institute, Busia, Kenya.
EClinicalMedicine. 2024 Feb 2;68:102454. doi: 10.1016/j.eclinm.2024.102454. eCollection 2024 Feb.
Viral load non-suppression (VLNS) in children is a major public health concern because of attendant HIV disease progression and risk of morbidity and mortality. Based on a nationally representative database we present estimates of the prevalence, trends and factors associated with VLNS in Kenyan pre-teenage children between 2015 and 2021.
Kenya National AIDS & STI Control Program's (NASCOP) maintains an early infant diagnosis and viral load (EID/VL) database for all persons living with HIV who are enrolled in the country's primary care clinics for purposes of monitoring progress towards achievement of the 95% viral suppression goals. Participants were eligible if they were children living with HIV (CLHIV), on combination ART (cART) treatment, and ≤12 years old. The modified Mann-Kendall trend test for serially correlated data was used to identify VLNS trends. Generalized estimating equations (GEE) with a logit link was used to assess the effects of covariates on the odds of VLNS (VL ≥1,000 copies/mL) over repeated points in time, allowing for the correlation among the repeated measures.
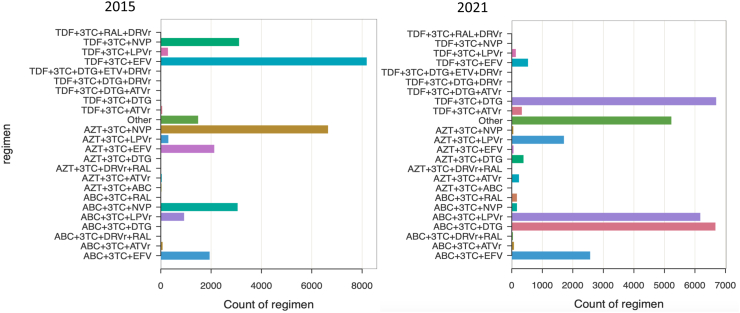
Between January 2015 and December 2021, 508,743 viral load tests were performed on samples collected from 109,682 pre-teenage children. The prevalence of VLNS decreased from 22.9% (95% CI 22.4-23.3) to 12.5% (95% CI 12.1-12.9), p < 0.0001, and mean age increased from 3.1 (4.2) to 8.0 (3.2) years in 2015 and 2021 respectively. A modified Mann-Kendall trend test for serially correlated data denotes a statistically significant decreasing trend (τ = -0.300, p < 0.0001) over the study period. In the multivariable GEE analysis adjusted for covariates, the odds of VLNS decreased by 11% per year during the study period, (GEE-aOR 0.89, 95% CI 0.88-0.90; p < 0.0001). Factors positively associated with VLNS were EFV/NVP-based first-line cART regimen (GEE-aOR 1.74, 95% CI 1.65-1.84, p < 0.0001), PI-based cART regimen (GEE-aOR 1.82, 95% CI 1.72-1.92, p < 0.0001), and children aged 1-3 years (toddlers) (GEE-aOR: 1.84, 95% CI 1.79-1.90, p < 0.0001). On the contrary, DTG-based cART regimen, were negatively associated with VLNS (GEE-aOR 0.70, 95% CI 0.65-0.75, p < 0.0001).
There is a strong evidence of decreasing viremia between 2015 and 2021. To sustain the decreasing trend, accelerating the switch from the suboptimal EVP/NVP first-line regimen to optimised DTG regimen is warranted.
U.S. President's Emergency Plan for AIDS Relief (PEPFAR) and Clinton Health Access Initiative (CHAI).
儿童病毒载量未被抑制(VLNS)是一个重大的公共卫生问题,因为这会导致艾滋病病情进展,并带来发病和死亡风险。基于一个具有全国代表性的数据库,我们给出了2015年至2021年肯尼亚青少年儿童中VLNS的患病率、趋势及相关因素的估计值。
肯尼亚国家艾滋病与性传播感染控制项目(NASCOP)为所有在该国初级保健诊所登记的艾滋病毒感染者维护一个早期婴儿诊断和病毒载量(EID/VL)数据库,以监测实现95%病毒抑制目标的进展情况。参与者若为感染艾滋病毒的儿童(CLHIV)、正在接受抗逆转录病毒联合治疗(cART)且年龄≤12岁,则符合条件。使用针对序列相关数据的改良曼-肯德尔趋势检验来确定VLNS趋势。使用具有logit链接的广义估计方程(GEE)来评估协变量在多个时间点上对VLNS(病毒载量≥1000拷贝/毫升)几率的影响,同时考虑重复测量之间的相关性。
2015年1月至2021年12月期间,对从109,682名青少年儿童采集的样本进行了508,743次病毒载量检测。VLNS的患病率从22.9%(95%置信区间22.4 - 23.3)降至12.5%(95%置信区间12.1 - 12.9),p < 0.0001,2015年和2021年的平均年龄分别从3.1(4.2)岁增至8.0(3.2)岁。针对序列相关数据的改良曼-肯德尔趋势检验表明,在研究期间存在统计学上显著的下降趋势(τ = -0.300,p < 0.0001)。在针对协变量进行调整的多变量GEE分析中,研究期间VLNS的几率每年下降11%,(GEE - aOR 0.89,95%置信区间0.88 - 0.90;p < 0.0001)。与VLNS呈正相关的因素包括基于依非韦伦/奈韦拉平的一线cART方案(GEE - aOR 1.74,95%置信区间1.65 - 1.84,p < 0.0001)、基于蛋白酶抑制剂的cART方案(GEE - aOR 1.82,95%置信区间1.72 - 1.92,p < 0.0001)以及1 - 3岁的儿童(幼儿)(GEE - aOR:1.84,95%置信区间1.79 - 1.90,p < 0.0001)。相反,基于多替拉韦的cART方案与VLNS呈负相关(GEE - aOR 0.70,95%置信区间0.65 - 0.75,p < 0.0001)。
有强有力的证据表明2015年至2021年期间病毒血症有所下降。为维持下降趋势,有必要加快从次优的依非韦伦/奈韦拉平一线方案转换为优化的多替拉韦方案。
美国总统艾滋病紧急救援计划(PEPFAR)和克林顿健康获取倡议组织(CHAI)。