Buzasi Eva, Carreira Helena, Funston Garth, Mansfield Kathryn E, Forbes Harriet, Strongman Helen, Bhaskaran Krishnan
Department of Non-Communicable Diseases Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Wolfson Institute of Population Health, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, UK.
Lancet Healthy Longev. 2024 Mar;5(3):e194-e203. doi: 10.1016/S2666-7568(23)00285-4. Epub 2024 Feb 6.
A history of multiple myeloma, prostate cancer, and breast cancer has been associated with adverse bone health, but associations across a broader range of cancers are unclear. We aimed to compare the risk of any bone fracture and major osteoporotic fractures in survivors of a wide range of cancers versus cancer-free individuals.
In this population-based matched cohort study, we used electronic health records from the UK Clinical Practice Research Datalink linked to hospital data. We included adults (aged ≥18 years) eligible for linkage, and we restricted the study start to Jan 2, 1998, onwards and applied administrative censoring on Jan 31, 2020. The cancer survivor group included survivors of the 20 most common cancers. Each individual with cancer was matched (age, sex, and general practice) to up to five controls (1:5) who were cancer-free. The primary outcomes were any bone fracture and any major osteoporotic fracture (pelvic, hip, wrist, spine, or proximal humeral fractures) occurring more than 1 year after index date (ie, the diagnosis date of the matched individual with cancer). We used Cox regression models, adjusted for shared risk factors, to estimate associations between cancer survivorship and bone fractures.
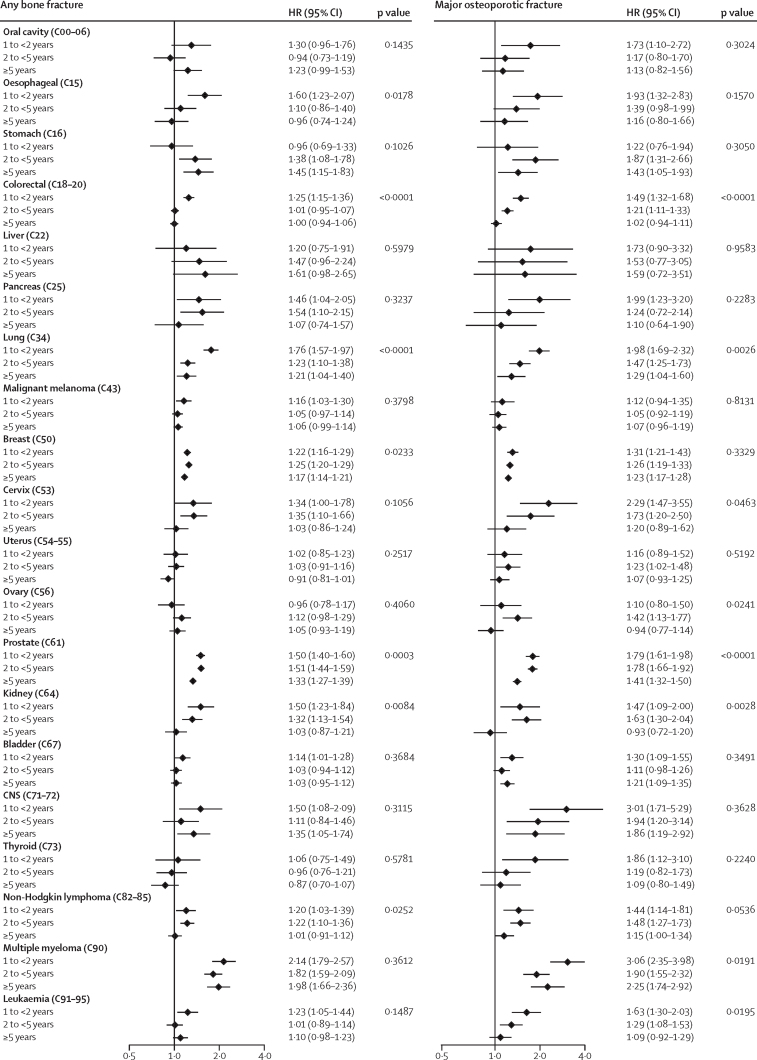
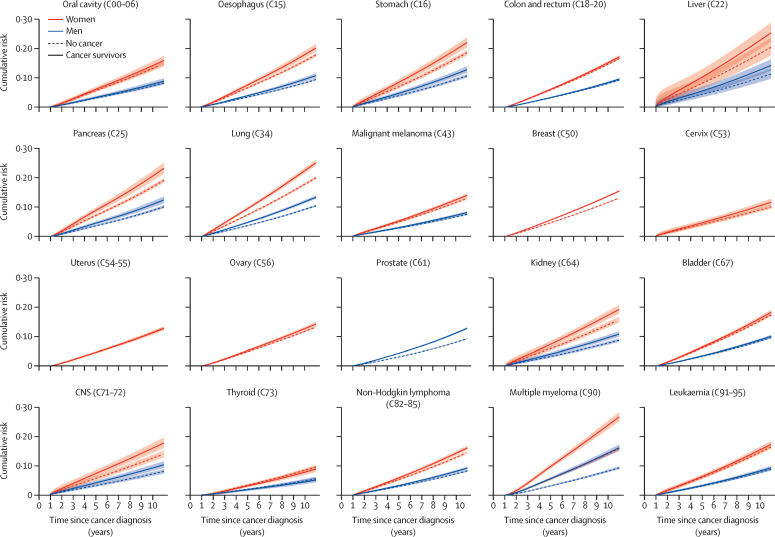
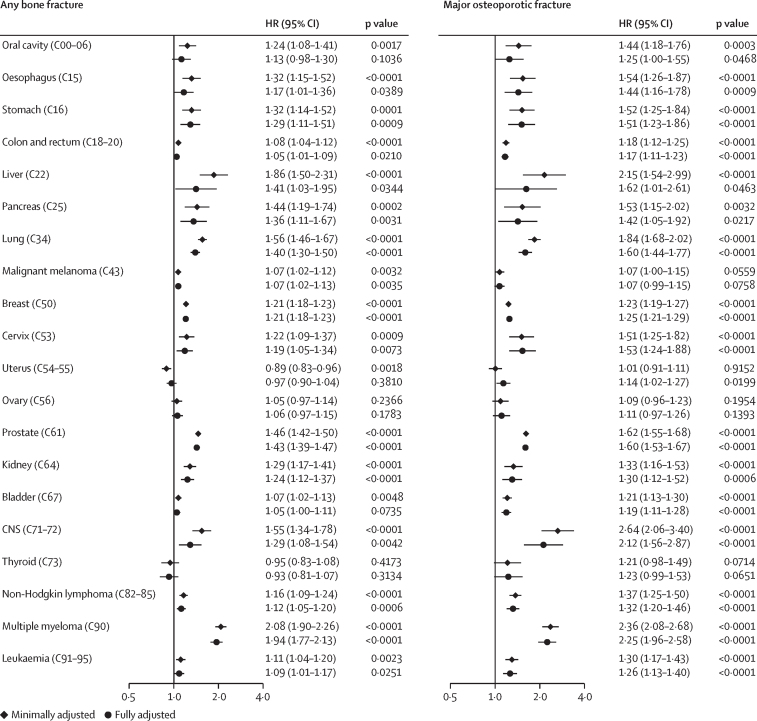
578 160 adults with cancer diagnosed in 1998-2020 were matched to 3 226 404 cancer-free individuals. Crude incidence rates of fractures in cancer survivors ranged between 8·39 cases (95% CI 7·45-9·46) per 1000 person-years for thyroid cancer and 21·62 cases (20·18-23·18) per 1000 person-years for multiple myeloma. Compared with cancer-free individuals, the risk of any bone fracture was increased in 15 of 20 cancers, and of major osteoporotic fractures in 17 of 20 cancers. Effect sizes varied: adjusted hazard ratios (HRs) were largest for multiple myeloma (1·94, 95% CI 1·77-2·13) and prostate cancer (1·43, 1·39-1·47); HRs in the range 1·20-1·50 were seen for stomach, liver, pancreas, lung, breast, kidney, and CNS cancers; smaller associations (HR <1·20) were observed for malignant melanoma, non-Hodgkin lymphoma, leukaemia, and oesophageal, colorectal, and cervical cancers. Increased risks of major osteoporotic fracture were noted most substantially in multiple myeloma (2·25, 1·96-2·58) and CNS (2·12, 1·56-2·87), liver (1·62, 1·01-2·61), prostate (1·60, 1·53-1·67), and lung cancers (1·60, 1·44-1·77). Effect sizes tended to reduce over time since diagnosis but remained elevated for more than 5 years in several cancers, such as multiple myeloma and stomach, lung, breast, prostate, and CNS cancers.
Survivors of most types of cancer were at increased risk of bone fracture for several years after cancer, with variation by cancer type. These findings can help to inform mitigation and prevention strategies.
Wellcome Trust.
多发性骨髓瘤、前列腺癌和乳腺癌病史与不良骨骼健康有关,但更广泛范围内癌症的关联尚不清楚。我们旨在比较广泛癌症幸存者与无癌个体发生任何骨折和严重骨质疏松性骨折的风险。
在这项基于人群的匹配队列研究中,我们使用了与医院数据相关联的英国临床实践研究数据链中的电子健康记录。我们纳入了符合关联条件的成年人(年龄≥18岁),并将研究开始时间限制在1998年1月2日及以后,并于2020年1月31日进行行政审查。癌症幸存者组包括20种最常见癌症的幸存者。每例癌症患者与多达5名无癌对照(1:5)进行匹配(年龄、性别和全科医疗)。主要结局是在索引日期(即匹配的癌症患者的诊断日期)后1年以上发生的任何骨折和任何严重骨质疏松性骨折(骨盆、髋部、腕部、脊柱或肱骨近端骨折)。我们使用Cox回归模型,并对共同风险因素进行调整,以估计癌症幸存者与骨折之间的关联。
1998 - 2020年诊断为癌症的578160名成年人与3226404名无癌个体进行了匹配。癌症幸存者骨折的粗发病率在甲状腺癌每1000人年8.39例(95%CI 7.45 - 9.46)至多发性骨髓瘤每1000人年21.62例(20.18 - 23.18)之间。与无癌个体相比,20种癌症中有15种发生任何骨折的风险增加,20种癌症中有17种发生严重骨质疏松性骨折的风险增加。效应大小各不相同:调整后的风险比(HR)在多发性骨髓瘤(1.94,95%CI 1.77 - 2.13)和前列腺癌(1.43,1.39 - 1.47)中最大;胃癌、肝癌、胰腺癌、肺癌、乳腺癌、肾癌和中枢神经系统癌症的HR在1.20 - 1.50范围内;恶性黑色素瘤、非霍奇金淋巴瘤、白血病以及食管癌、结直肠癌和宫颈癌的关联较小(HR <1.20)。严重骨质疏松性骨折风险增加在多发性骨髓瘤(2.25,1.96 - 2.58)、中枢神经系统癌症(2.12,1.56 - 2.87)、肝癌(1.62,1.01 - 2.61)、前列腺癌(1.60,1.53 - 1.67)和肺癌(1.60,1.44 - 1.77)中最为显著。自诊断以来,效应大小往往随时间降低,但在几种癌症中,如多发性骨髓瘤、胃癌、肺癌、乳腺癌、前列腺癌和中枢神经系统癌症中,5年以上仍保持升高。
大多数类型癌症的幸存者在癌症发生后的几年内骨折风险增加,且因癌症类型而异。这些发现有助于为缓解和预防策略提供信息。
惠康信托基金会。