Cardiovascular Department, Cliniques universitaires Saint-Luc, Brussels, Belgium.
Pôle de Recherche Cardiovasculaire (CARD), Institut de Recherche Expérimentale et Clinique (IREC), Université Catholique de Louvain (UCLouvain), Brussels, Belgium.
ESC Heart Fail. 2024 Jun;11(3):1493-1505. doi: 10.1002/ehf2.14699. Epub 2024 Feb 9.
Heart failure (HF) with preserved ejection fraction (HFpEF) is a disease associated with high morbidity and mortality, for which it is difficult to identify patients with the poorest prognosis in routine clinical practice. Carbohydrate antigen 125 (CA 125) has been shown to be a potential marker of congestion and prognosis in HF. We sought to better characterize HFpEF patients with high CA 125 levels by using a multimodal approach.
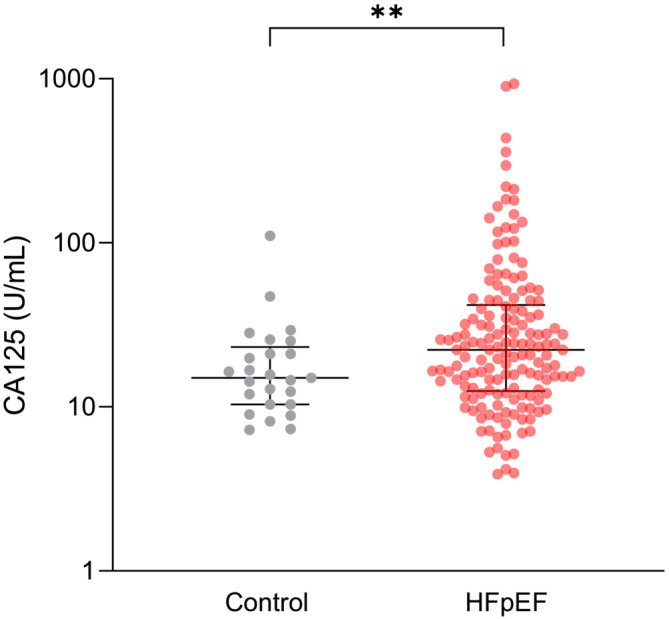
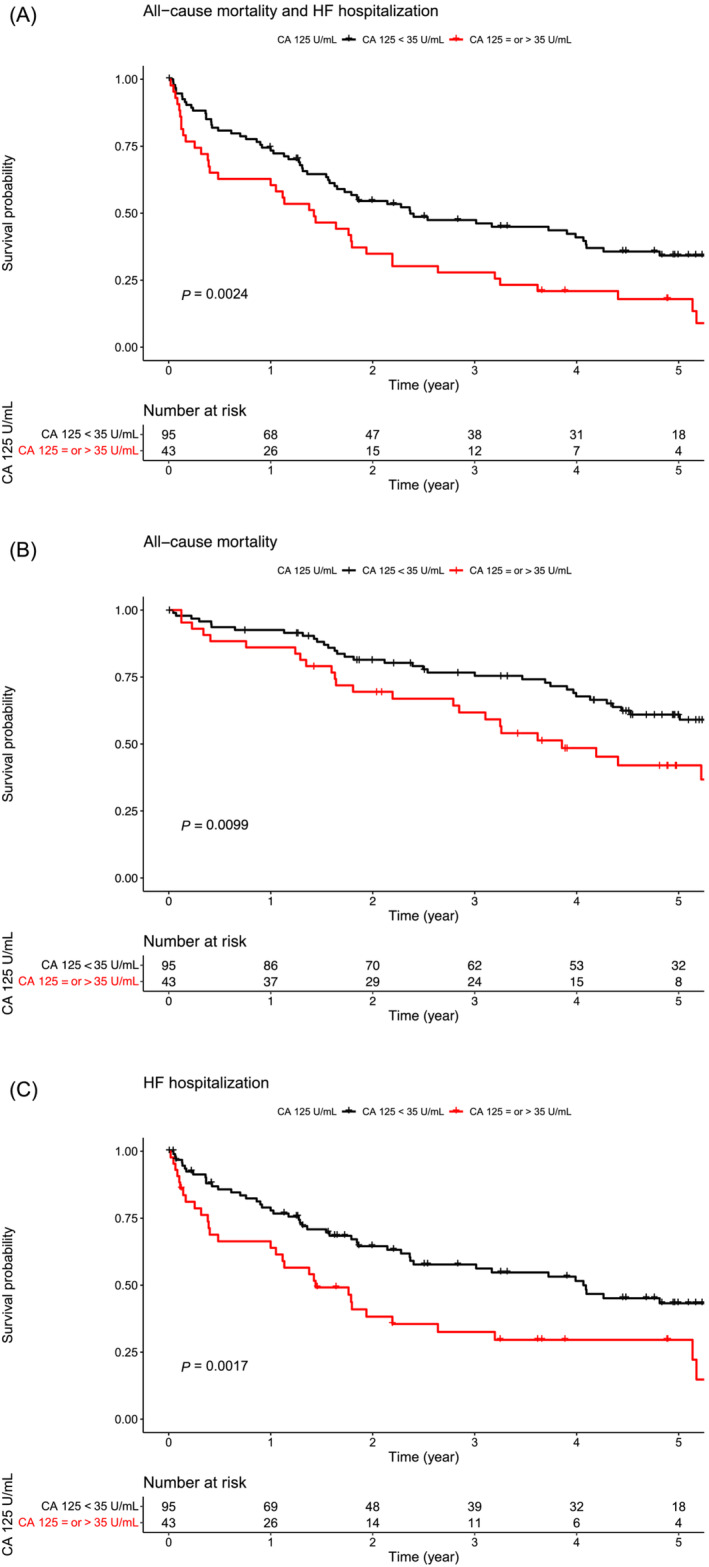
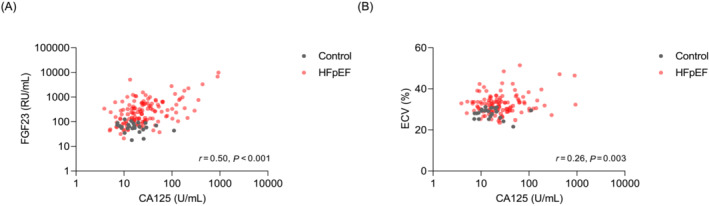
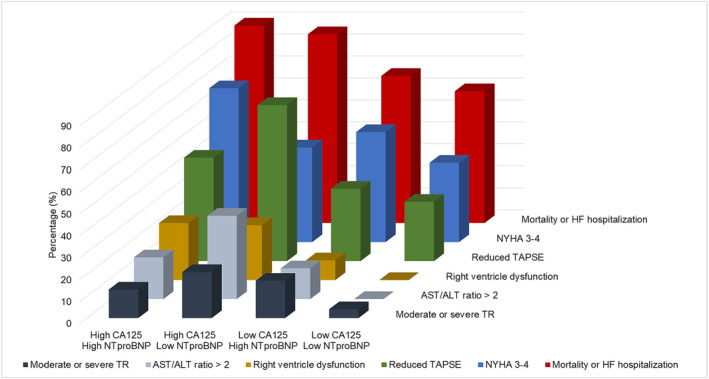
We prospectively enrolled 139 HFpEF patients (78 ± 8 years; 60% females) and 25 controls matched for age and sex (77 ± 5 years; 60% females). They underwent two-dimensional echocardiography, cardiac magnetic resonance with late gadolinium enhancement [including extracellular volume (ECV) measurement], and serum measurements of CA 125 level. The primary endpoint of the study was a composite of all-cause mortality or first HF hospitalization. The prognostic impact of CA 125 was determined using Cox proportional hazard models. Median CA 125 levels were significantly higher in HFpEF patients compared with controls [CA 125: 23.5 (14.5-44.7) vs. 14.6 (10.3-21.0) U/mL, P = 0.004]. CA 125 levels were positively correlated with a congestion marker [N-terminal pro-brain natriuretic peptide (NT-proBNP) levels, Pearson's r = 0.37, P < 0.001] and markers of cardiac fibrosis estimated by both ECV (Pearson's r = 0.26, P = 0.003) and fibroblast growth factor 23 levels (Pearson's r = 0.50, P < 0.001). Over a median follow-up of 49 (22-64) months, 97 HFpEF patients reached the composite endpoint. Even after adjustment for the Meta-Analysis Global Group in Chronic risk score, a CA 125 level ≥35 U/mL was still a significant predictor of the composite endpoint [hazard ratio (HR): 1.58 (1.04-2.41), P = 0.032] and more particularly of HF hospitalization [HR: 1.81 (1.13-2.92), P = 0.014]. In contrast, NT-proBNP levels were not an independent predictor.
CA 125 levels were significantly higher in HFpEF patients compared with controls matched for age and sex and were associated with markers of congestion and cardiac fibrosis. CA 125 levels were a strong and independent predictor of HF hospitalization in HFpEF patients. These data suggest a potential value of CA 125 as a biomarker for staging and risk prediction in HFpEF.
射血分数保留的心力衰竭(HFpEF)是一种与高发病率和死亡率相关的疾病,在常规临床实践中很难识别预后最差的患者。糖链抗原 125(CA 125)已被证明是心力衰竭充血和预后的潜在标志物。我们试图通过多模态方法更好地描述 CA 125 水平较高的 HFpEF 患者。
我们前瞻性纳入了 139 例 HFpEF 患者(78±8 岁;60%为女性)和 25 例年龄和性别匹配的对照者(77±5 岁;60%为女性)。他们接受了二维超声心动图、心脏磁共振检查(包括钆延迟增强[包括细胞外容积(ECV)测量])和血清 CA 125 水平检测。研究的主要终点是全因死亡率或首次心力衰竭住院的复合终点。使用 Cox 比例风险模型确定 CA 125 的预后影响。HFpEF 患者的 CA 125 水平明显高于对照组[CA 125:23.5(14.5-44.7)vs. 14.6(10.3-21.0)U/mL,P=0.004]。CA 125 水平与充血标志物[N 末端脑利钠肽前体(NT-proBNP)水平呈正相关(Pearson r=0.37,P<0.001)]和通过 ECV(Pearson r=0.26,P=0.003)和成纤维细胞生长因子 23 水平(Pearson r=0.50,P<0.001)估计的心脏纤维化标志物呈正相关。在中位随访 49(22-64)个月期间,97 例 HFpEF 患者达到了复合终点。即使在调整 Meta-Analysis Global Group in Chronic 风险评分后,CA 125 水平≥35 U/mL 仍然是复合终点的显著预测因子[风险比(HR):1.58(1.04-2.41),P=0.032],特别是心力衰竭住院的预测因子[HR:1.81(1.13-2.92),P=0.014]。相比之下,NT-proBNP 水平不是独立的预测因子。
HFpEF 患者的 CA 125 水平明显高于年龄和性别匹配的对照组,与充血和心脏纤维化标志物相关。CA 125 水平是 HFpEF 患者心力衰竭住院的强独立预测因子。这些数据表明 CA 125 作为 HFpEF 分期和风险预测的生物标志物具有潜在价值。