Gu Jun, Wang Yue, Zhang Jun-Feng, Wang Chang-Qian
Department of Cardiology, Shanghai Ninth People's Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People's Republic of China.
Int J Cardiol Heart Vasc. 2024 Feb 6;50:101353. doi: 10.1016/j.ijcha.2024.101353. eCollection 2024 Feb.
Although prophylactic anticoagulation therapy is suggested to be adopted in severe COVID-19 patients, its effects on the long-term cardiovascular (CV) outcomes, namely the risk of major adverse CV events(MACEs) in high-risk CV patients amid the omicron wave of the pandemic, remain unknown.
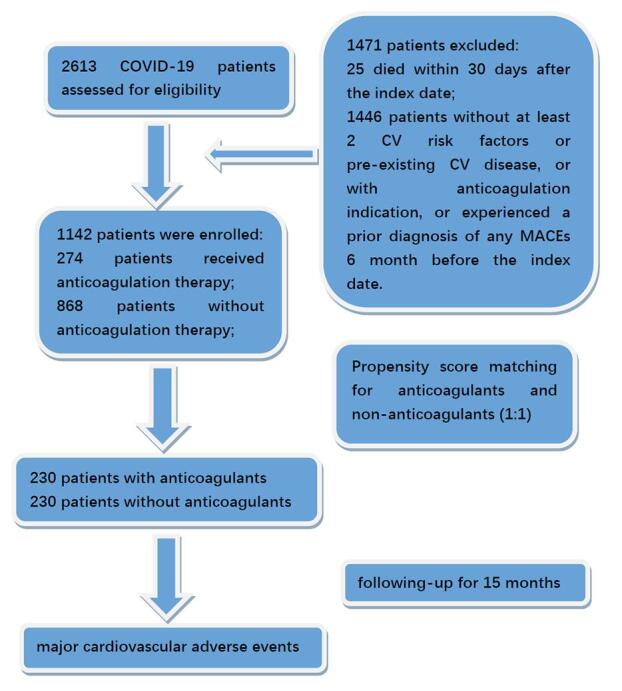
We conducted this prospective cohort study of consecutive adults hospitalized COVID-19 between 19 April and 12 June 2022, COVID-19 patients with at least two CV risk factors or pre-existing CV diseases were enrolled. A propensity score matching(PSM) method was used to evaluated the effects of prophylactic anticoagulation therapy in hospital on long-term MACEs, including CV death, non-fatal myocardial infarction, non-fatal stroke, hospitalization due to unstable angina pectoris, coronary revascularization and arterial or venous thrombosis.
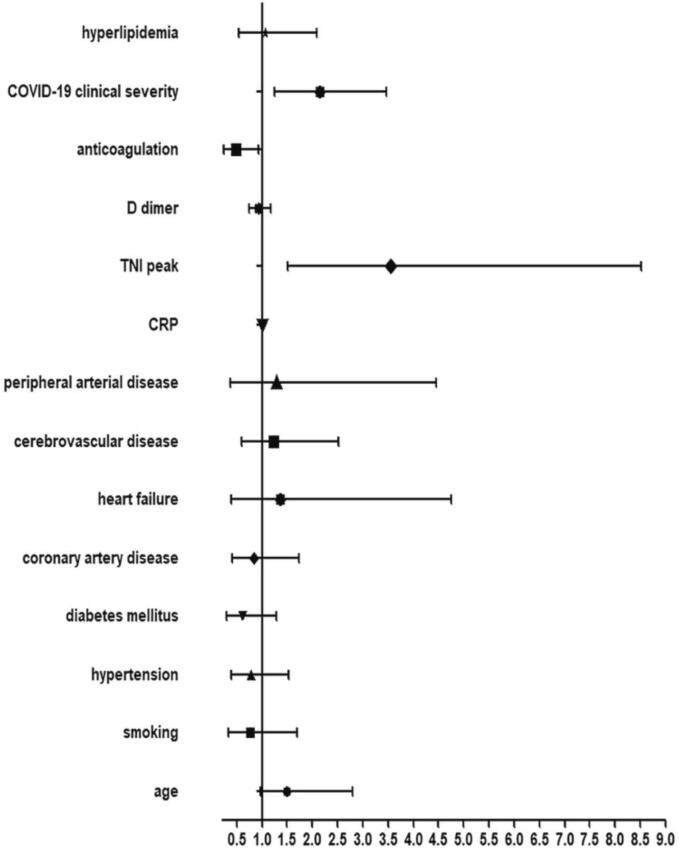
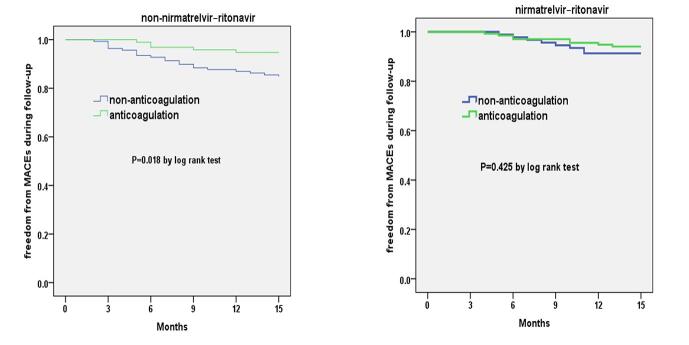
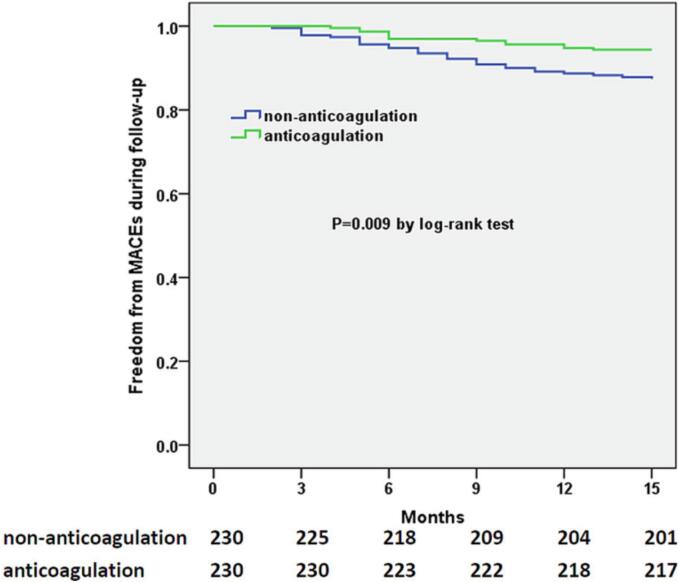
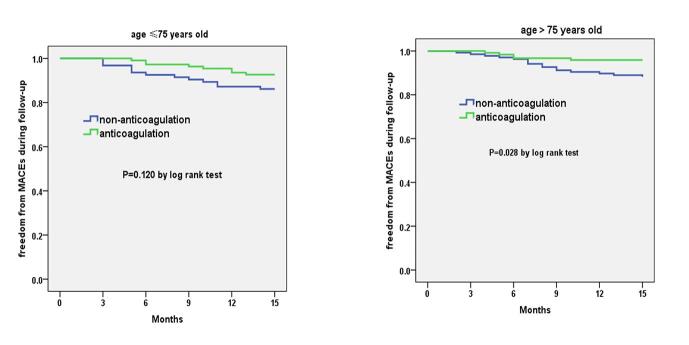
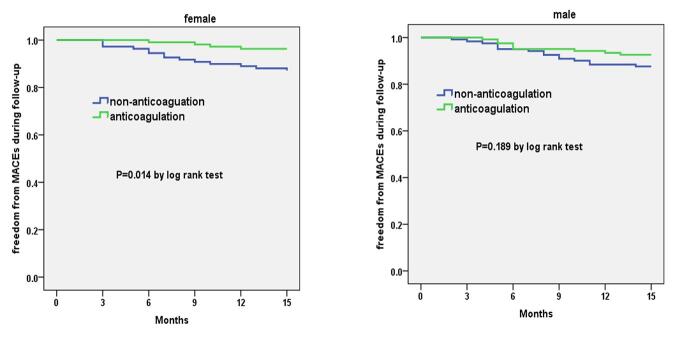
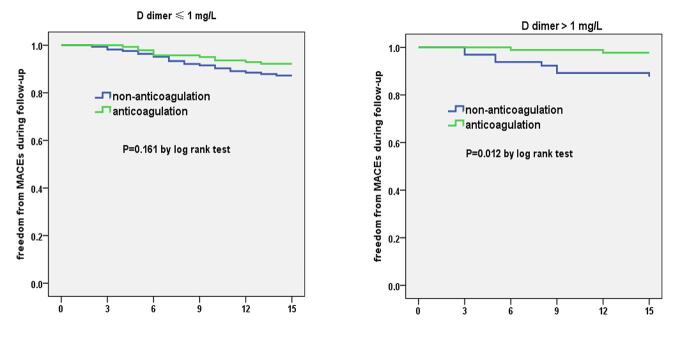
Two cohorts (with or without anticoagulants during hospitalization) of each 230 patients with balanced baseline characteristics were formed using PSM. During the 15-month follow-up period, 13 patients with anticoagulants and 29 patients without anticoagulants developed MACEs. Overall, the anticoagulation group had a significantly lower risk of MACEs than the control group (hazard ratio [HR] 0.431; 95 % confidence interval [CI]: 0.224-0.830, P = 0.010). Regarding specific constituents of MACEs, the differences were mainly reflected in arterial or venous thrombosis. The significantly lower HRs of overall MACEs were significantly observed in subgroup of age > 75 years, women, higher D dimer level, unvaccinated and non-nirmatrelvir-ritonavir prescribed patients.
Prophylactic anticoagulation therapy during hospitalization was effective in reducing long-term MACEs among COVID-19 patients with CV risk factors or pre-existing CV diseases amid the omicron wave of the pandemic.
尽管建议对重症新型冠状病毒肺炎(COVID-19)患者采用预防性抗凝治疗,但其对长期心血管(CV)结局的影响,即在疫情奥密克戎毒株流行期间高危CV患者发生主要不良心血管事件(MACE)的风险,仍不清楚。
我们对2022年4月19日至6月12日期间连续住院的成年COVID-19患者进行了这项前瞻性队列研究,纳入了至少有两个CV危险因素或既往有CV疾病的COVID-19患者。采用倾向评分匹配(PSM)方法评估住院期间预防性抗凝治疗对长期MACE的影响,包括CV死亡、非致命性心肌梗死、非致命性卒中、不稳定型心绞痛住院、冠状动脉血运重建以及动脉或静脉血栓形成。
使用PSM形成了两个队列(住院期间使用或未使用抗凝剂),每组230例患者,基线特征均衡。在15个月的随访期内,使用抗凝剂的患者中有13例发生MACE,未使用抗凝剂的患者中有29例发生MACE。总体而言,抗凝组发生MACE的风险显著低于对照组(风险比[HR]0.431;95%置信区间[CI]:0.224-0.830,P = 0.010)。关于MACE的具体组成部分,差异主要体现在动脉或静脉血栓形成方面。在年龄>75岁、女性、D-二聚体水平较高、未接种疫苗以及未使用奈玛特韦-利托那韦的患者亚组中,总体MACE的HR显著较低。
在疫情奥密克戎毒株流行期间,住院期间的预防性抗凝治疗可有效降低有CV危险因素或既往有CV疾病的COVID-19患者的长期MACE。