Department of Pathology, Louisiana State University Health Sciences Center, 7th Floor, 2021 Perdido Street, New Orleans, Louisiana, 70112, USA.
Department of Pathology, Virginia Commonwealth University, Norfolk, Virginia, 23510, USA.
Diagn Pathol. 2024 Feb 15;19(1):33. doi: 10.1186/s13000-024-01445-w.
Hypercytokinemia, the renin-angiotensin system, hypoxia, immune dysregulation, and vasculopathy with evidence of immune-related damage are implicated in brain morbidity in COVID-19 along with a wide variety of genomic and environmental influences. There is relatively little evidence of direct SARS-CoV-2 brain infection in COVID-19 patients.
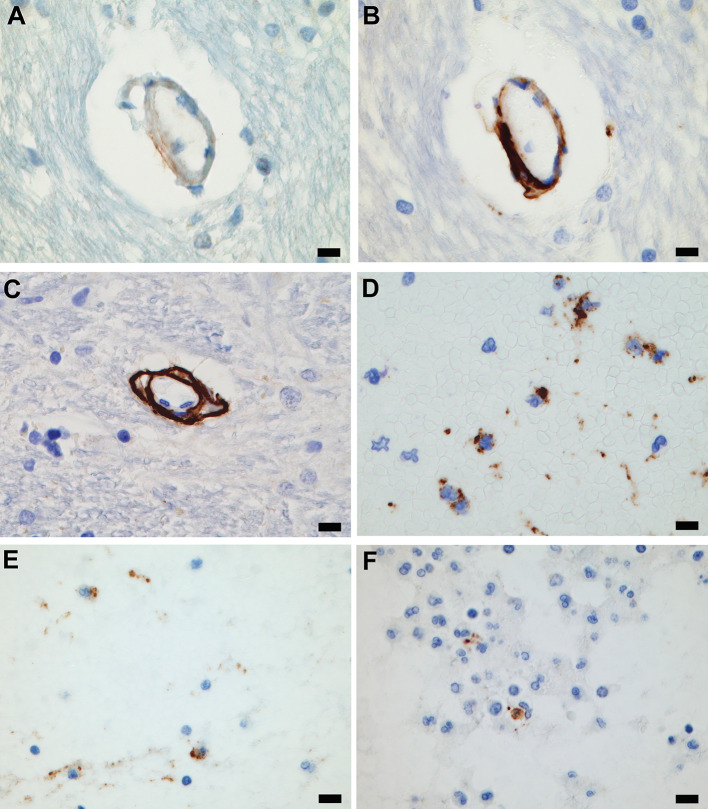
Brain histopathology of 36 consecutive autopsies of patients who were RT-PCR positive for SARS-CoV-2 was studied along with findings from contemporary and pre-pandemic historical control groups. Immunostaining for serum and blood cell proteins and for complement components was employed. Microcirculatory wall complement deposition in the COVID-19 cohort was compared to historical control cases. Comparisons also included other relevant clinicopathological and microcirculatory findings in the COVID-19 cohort and control groups.
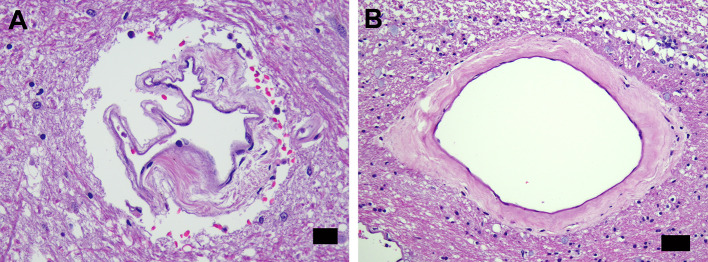
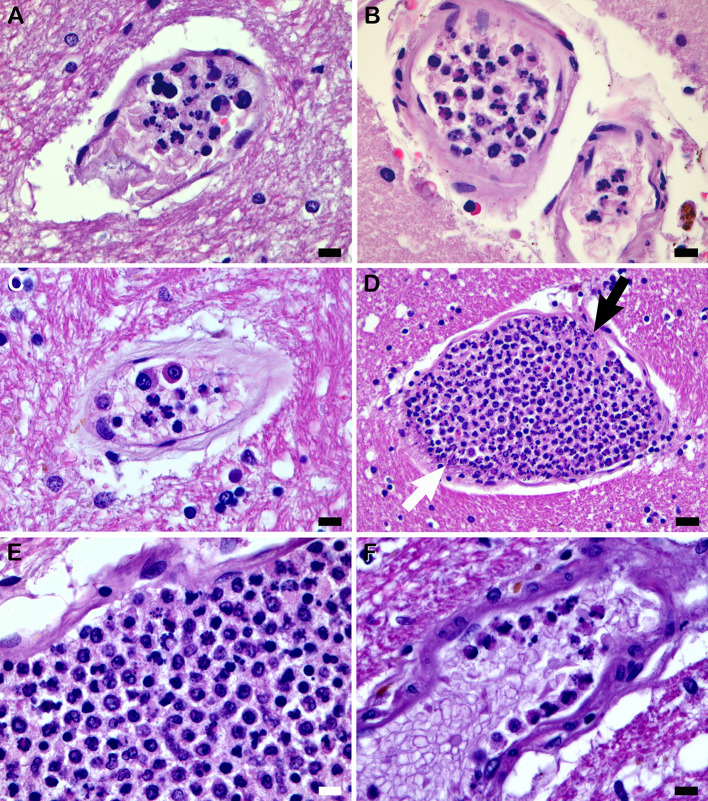
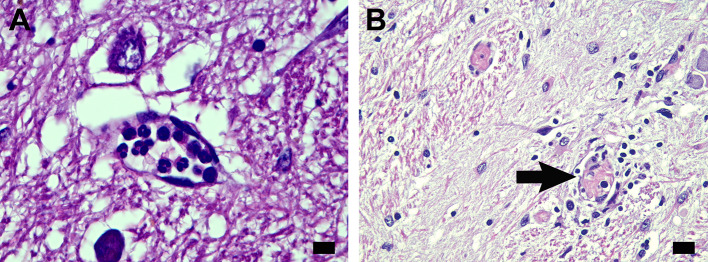
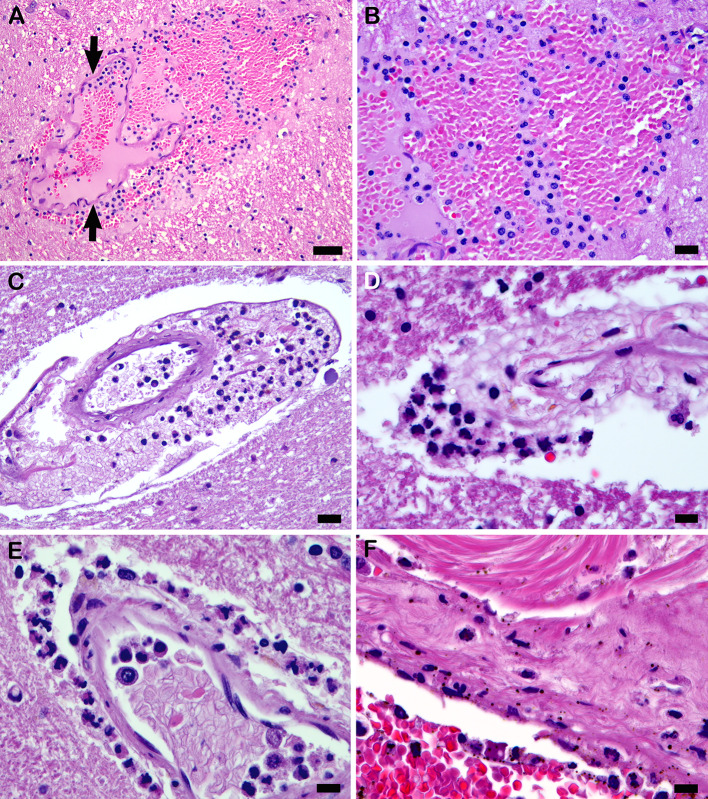
The COVID-19 cohort and both the contemporary and historical control groups had the same rate of hypertension, diabetes mellitus, and obesity. The COVID-19 cohort had varying amounts of acute neutrophilic vasculitis with leukocytoclasia in the microcirculation of the brain in all cases. Prominent vascular neutrophilic transmural migration was found in several cases and 25 cases had acute perivasculitis. Paravascular microhemorrhages and petechial hemorrhages (small brain parenchymal hemorrhages) had a slight tendency to be more numerous in cohort cases that displayed less acute neutrophilic vasculitis. Tissue burden of acute neutrophilic vasculitis with leukocytoclasia was the same in control cases as a group, while it was significantly higher in COVID-19 cases. Both the tissue burden of acute neutrophilic vasculitis and the activation of complement components, including membrane attack complex, were significantly higher in microcirculatory channels in COVID-19 cohort brains than in historical controls.
Acute neutrophilic vasculitis with leukocytoclasia, acute perivasculitis, and associated paravascular blood extravasation into brain parenchyma constitute the first phase of an immune-related, acute small-vessel inflammatory condition often termed type 3 hypersensitivity vasculitis or leukocytoclastic vasculitis. There is a higher tissue burden of acute neutrophilic vasculitis and an increased level of activated complement components in microcirculatory walls in COVID-19 cases than in pre-pandemic control cases. These findings are consistent with a more extensive small-vessel immune-related vasculitis in COVID-19 cases than in control cases. The pathway(s) and mechanism for these findings are speculative.
细胞因子血症、肾素-血管紧张素系统、缺氧、免疫失调和血管病变伴有免疫相关损伤,这些都与 COVID-19 患者的大脑发病机制有关,同时还受到多种基因组和环境因素的影响。在 COVID-19 患者中,很少有直接的 SARS-CoV-2 脑感染的证据。
对 36 例 RT-PCR 检测为 SARS-CoV-2 阳性的连续尸检患者的脑组织病理学进行了研究,并与同期和大流行前的历史对照组的结果进行了比较。使用血清和血细胞蛋白以及补体成分的免疫染色进行研究。比较了 COVID-19 队列中微脉管壁补体沉积与历史对照组病例。比较还包括 COVID-19 队列和对照组中的其他相关临床病理和微循环发现。
COVID-19 队列和同期及历史对照组的高血压、糖尿病和肥胖的发生率相同。在所有病例中,COVID-19 队列的大脑微循环中均存在不同程度的急性中性粒细胞性血管炎伴白细胞碎裂。在几个病例中发现了明显的血管中性粒细胞跨壁迁移,25 例有急性血管周围炎。血管周围微出血和瘀点(脑实质小出血)在显示较少急性中性粒细胞性血管炎的病例中数量略有增加。作为一个整体,对照组的急性中性粒细胞性血管炎伴白细胞碎裂的组织负担与对照组相同,而 COVID-19 病例的组织负担明显更高。COVID-19 队列脑微脉管中的急性中性粒细胞性血管炎和补体成分(包括膜攻击复合物)的组织负担均明显高于历史对照组。
伴有白细胞碎裂的急性中性粒细胞性血管炎、急性血管周围炎以及相关的血管周围血液渗出到脑实质中,构成了一种免疫相关的急性小血管炎症状态的第一阶段,通常称为 3 型超敏反应性血管炎或白细胞碎裂性血管炎。与大流行前对照组病例相比,COVID-19 病例的微脉管壁中急性中性粒细胞性血管炎的组织负担更高,激活的补体成分水平也更高。这些发现与 COVID-19 病例中比对照组更广泛的小血管免疫相关血管炎一致。这些发现的途径和机制仍有待推测。