Department of Stereotactic and Functional Neurosurgery, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany.
Department of Stereotactic and Functional Neurosurgery, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg im Breisgau, Germany.
Neuroimage Clin. 2024;41:103576. doi: 10.1016/j.nicl.2024.103576. Epub 2024 Feb 12.
Thalamic deep brain stimulation (DBS) is an efficacious treatment for drug-resistant essential tremor (ET) and the dentato-rubro-thalamic tract (DRT) constitutes an important target structure. However, up to 40% of patients habituate and lose treatment efficacy over time, frequently accompanied by a stimulation-induced cerebellar syndrome. The phenomenon termed delayed therapy escape (DTE) is insufficiently understood. Our previous work showed that DTE clinically is pronounced on the non-dominant side and suggested that differential involvement of crossed versus uncrossed DRT (DRTx/DRTu) might play a role in DTE development.
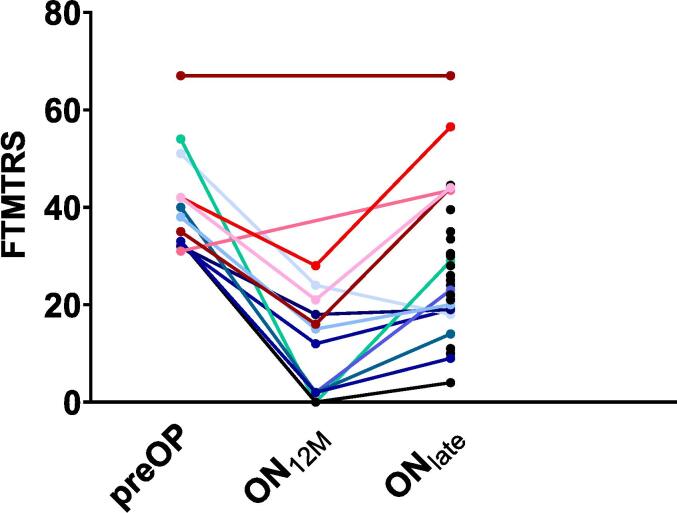
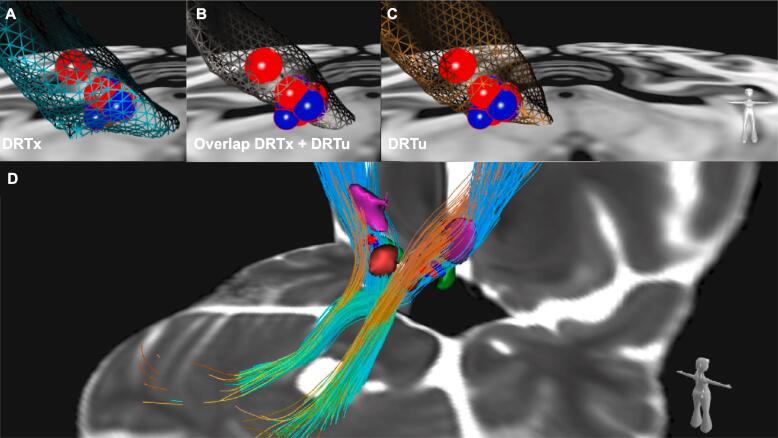
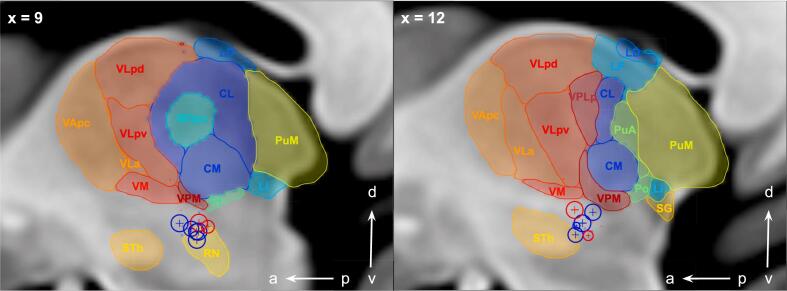
We retrospectively enrolled right-handed patients under bilateral thalamic DBS >12 months for ET from a cross-sectional study. They were characterized with the Fahn-Tolosa-Marin Tremor Rating Scale (FTMTRS) and Scale for the Assessment and Rating of Ataxia (SARA) scores at different timepoints. Normative fiber tractographic evaluations of crossed and uncrossed cerebellothalamic pathways and volume of activated tissue (VAT) studies together with [F]Fluorodeoxyglucose positron emission tomography were applied.
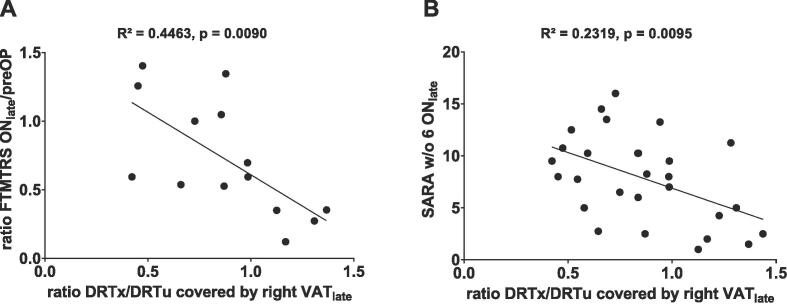
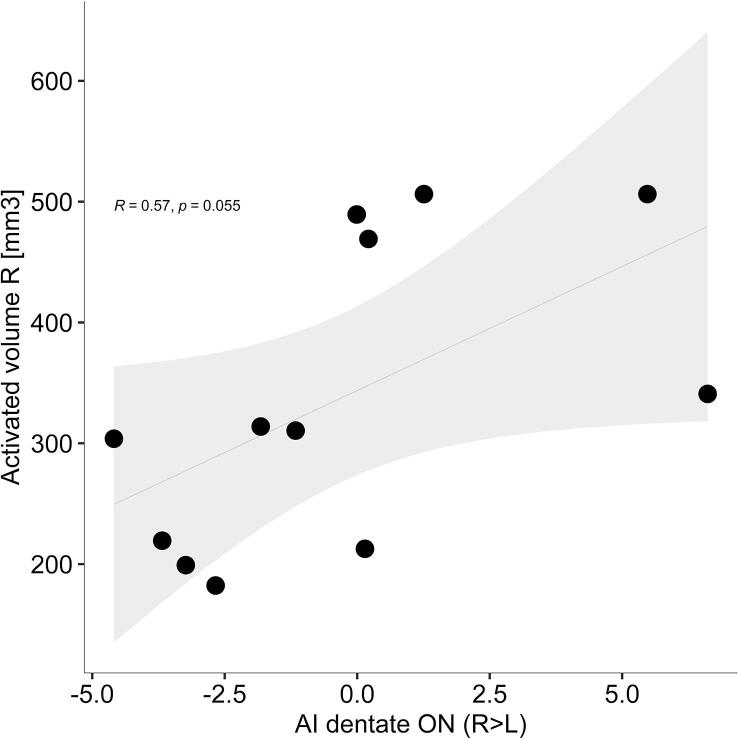
A total of 29 patients met the inclusion criteria. Favoring DRTu over DRTx in the non-dominant VAT was associated with DTE (R = 0.4463, p < 0.01) and ataxia (R = 0.2319, p < 0.01). Moreover, increasing VAT size on the right (non-dominant) side was associated at trend level with more asymmetric glucose metabolism shifting towards the right (dominant) dentate nucleus.
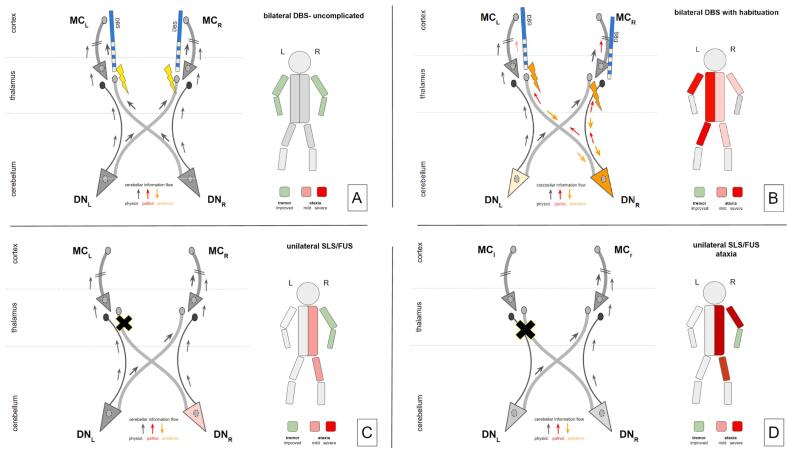
Our results suggest that a disbalanced recruitment of DRTu in the non-dominant VAT induces detrimental stimulation effects on the dominant cerebellar outflow (together with contralateral stimulation) leading to DTE and thus hampering the overall treatment efficacy.
丘脑深部脑刺激(DBS)是治疗耐药性原发性震颤(ET)的有效方法,齿状核红核丘脑束(DRT)构成了重要的靶结构。然而,多达 40%的患者随着时间的推移会习惯并失去治疗效果,常常伴有刺激诱导的小脑综合征。这种被称为延迟治疗逃逸(DTE)的现象尚未得到充分理解。我们之前的工作表明,DTE 在临床上在非优势侧更为明显,并表明交叉与未交叉 DRT(DRTx/DRTu)的差异参与可能在 DTE 发展中起作用。
我们从一项横断面研究中回顾性招募了右侧丘脑 DBS 治疗 ET 超过 12 个月的右利手患者。他们在不同时间点使用 Fahn-Tolosa-Marin 震颤评定量表(FTMTRS)和共济失调评定量表(SARA)进行了特征描述。应用了交叉和未交叉小脑丘脑通路的规范纤维束成像评估以及激活组织体积(VAT)研究,以及 [F]氟脱氧葡萄糖正电子发射断层扫描。
共有 29 名患者符合纳入标准。非优势侧 VAT 中 DRTu 优于 DRTx 与 DTE(R=0.4463,p<0.01)和共济失调(R=0.2319,p<0.01)有关。此外,右侧(非优势侧)VAT 大小的增加与右侧(优势侧)齿状核葡萄糖代谢向右侧转移的不对称性增加呈趋势相关。
我们的结果表明,非优势侧 VAT 中 DRTu 的不平衡募集会对优势侧小脑传出(与对侧刺激一起)产生有害的刺激效应,导致 DTE,从而损害整体治疗效果。