Department of Radiation Oncology, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan.
Program in Artificial Intelligence in Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Sci Rep. 2024 Feb 18;14(1):4011. doi: 10.1038/s41598-024-54369-2.
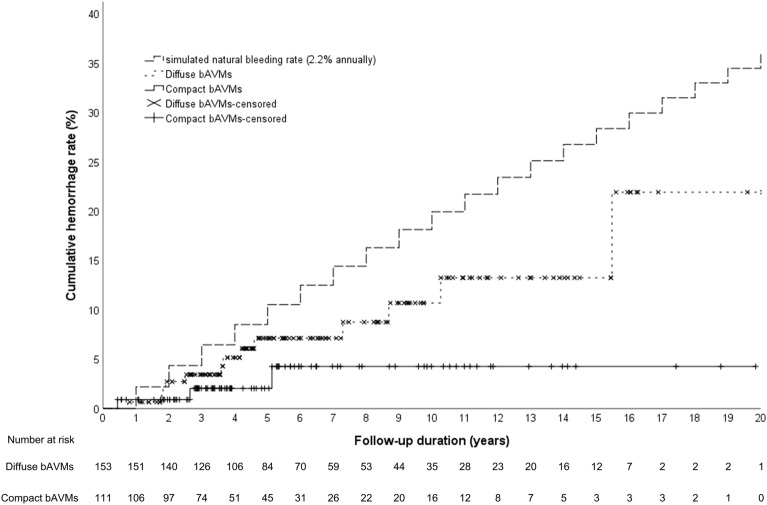
The aim of the study was to investigate whether morphology (i.e. compact/diffuse) of brain arteriovenous malformations (bAVMs) correlates with the incidence of hemorrhagic events in patients receiving Stereotactic Radiosurgery (SRS) for unruptured bAVMs. This retrospective study included 262 adult patients with unruptured bAVMs who underwent upfront SRS. Hemorrhagic events were defined as evidence of blood on CT or MRI. The morphology of bAVMs was evaluated using automated segmentation which calculated the proportion of vessel, brain tissue, and cerebrospinal fluid in bAVMs on T2-weighted MRI. Compactness index, defined as the ratio of vessel to brain tissue, categorized bAVMs into compact and diffuse types based on the optimal cutoff. Cox proportional hazard model was used to identify the independent factors for post-SRS hemorrhage. The median clinical follow-ups was 62.1 months. Post-SRS hemorrhage occurred in 13 (5.0%) patients and one of them had two bleeds, resulting in an annual bleeding rate of 0.8%. Multivariable analysis revealed bAVM morphology (compact versus diffuse), bAVM volume, and prescribed margin dose were significant predictors. The post-SRS hemorrhage rate increased with larger bAVM volume only among the diffuse nidi (1.7 versus 14.9 versus 30.6 hemorrhage per 1000 person-years in bAVM volume < 20 cm versus 20-40 cm versus > 40 cm; p = 0.022). The significantly higher post-SRS hemorrhage rate of Spetzler-Martin grade IV-V compared with grade I-III bAVMs (20.0 versus 3.3 hemorrhages per 1000 person-years; p = 0.001) mainly originated from the diffuse bAVMs rather than the compact subgroup (30.9 versus 4.8 hemorrhages per 1000 person-years; p = 0.035). Compact and smaller bAVMs, with higher prescribed margin dose harbor lower risks of post-SRS hemorrhage. The post-SRS hemorrhage rate exceeded 2.2% annually within the diffuse and large (> 40 cm) bAVMs and the diffuse Spetzler-Martin IV-V bAVMs. These findings may help guide patient selection of SRS for the unruptured bAVMs.
本研究旨在探讨接受立体定向放射外科 (SRS) 治疗的未破裂脑动静脉畸形 (bAVM) 患者,其 bAVM 的形态(致密型/弥漫型)是否与出血事件的发生相关。本回顾性研究纳入了 262 例接受初始 SRS 治疗的未破裂 bAVM 成年患者。出血事件定义为 CT 或 MRI 上有出血证据。bAVM 的形态使用自动分割进行评估,该方法计算 T2 加权 MRI 上 bAVM 中血管、脑组织和脑脊液的比例。致密指数定义为血管与脑组织的比值,根据最佳截断值将 bAVM 分为致密型和弥漫型。Cox 比例风险模型用于确定 SRS 后出血的独立因素。中位临床随访时间为 62.1 个月。SRS 后有 13 例(5.0%)患者发生出血,其中 1 例发生 2 次出血,年出血率为 0.8%。多变量分析显示,bAVM 形态(致密型与弥漫型)、bAVM 体积和预设边缘剂量是显著的预测因素。仅在弥漫性 nidi 中,随着 bAVM 体积的增大,SRS 后出血率增加(bAVM 体积 < 20 cm、20-40 cm 和 > 40 cm 时的每年出血率分别为 1.7、14.9 和 30.6 出血/1000 人年;p=0.022)。与 Spetzler-Martin 分级 I-III 相比,Spetzler-Martin 分级 IV-V 的 bAVM 的 SRS 后出血率显著更高(20.0 与 3.3 出血/1000 人年;p=0.001),主要来源于弥漫性 bAVM,而非致密型亚组(30.9 与 4.8 出血/1000 人年;p=0.035)。致密型和较小的 bAVM,以及较高的预设边缘剂量,其 SRS 后出血风险较低。弥漫性和较大 (> 40 cm) bAVM 以及弥漫性 Spetzler-Martin IV-V bAVM 的 SRS 后出血率每年超过 2.2%。这些发现可能有助于指导未破裂 bAVM 的 SRS 患者选择。