Zhang Panpan, Ma Minting, Nie Jun, Dai Ling, Hu Weiheng, Zhang Jie, Wu Di, Chen Xiaoling, Ma Xiangjuan, Tian Guangming, Han Sen, Long Jieran, Wang Yang, Zhang Ziran, Hao Qianyun, Fang Jian
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Thoracic Oncology II, Peking University Cancer Hospital and Institute, Beijing, China.
Department of Oncology, The Fourth Hospital of Hebei Medical University, Shijiazhuang, China.
Heliyon. 2024 Feb 11;10(4):e26026. doi: 10.1016/j.heliyon.2024.e26026. eCollection 2024 Feb 29.
The purpose of this study is to investigate the efficacy and safety of immune checkpoint inhibitors (ICIs) or plus with chemotherapy in older patients.
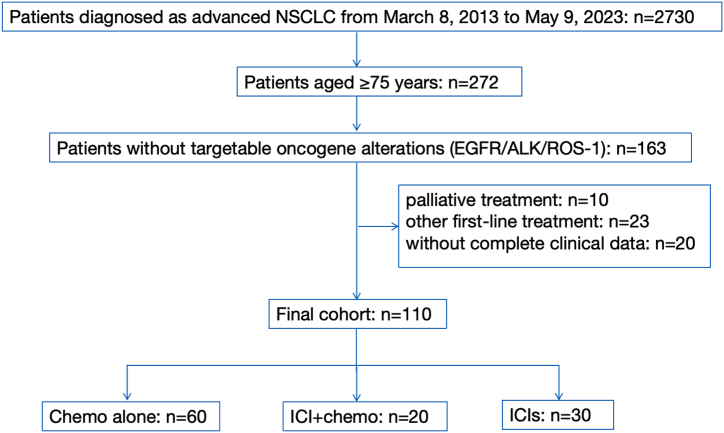
We enrolled 110 older patients with non-small cell lung cancer (NSCLC ≥75 years) who received either chemotherapy alone (chemo), ICI plus chemotherapy (ICI + chemo), or ICI alone and ICI plus other therapies, which included anti-angiogenesis drugs or other novel ICI (ICIs). Patient characteristics, treatment response, survival, and toxicity were evaluated.
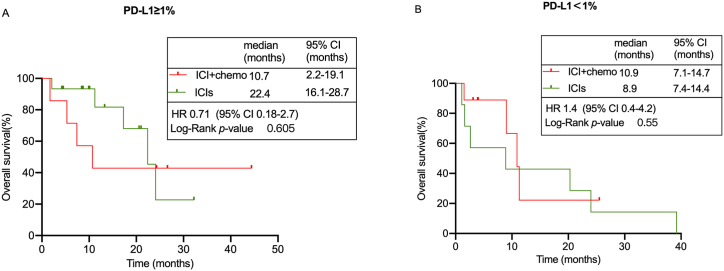
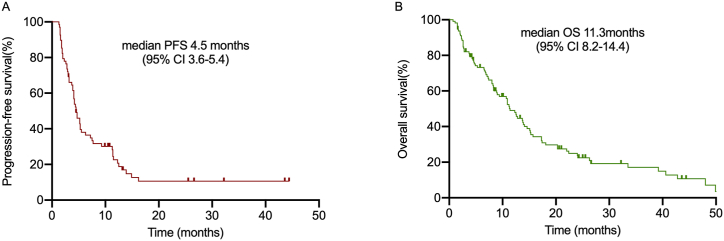
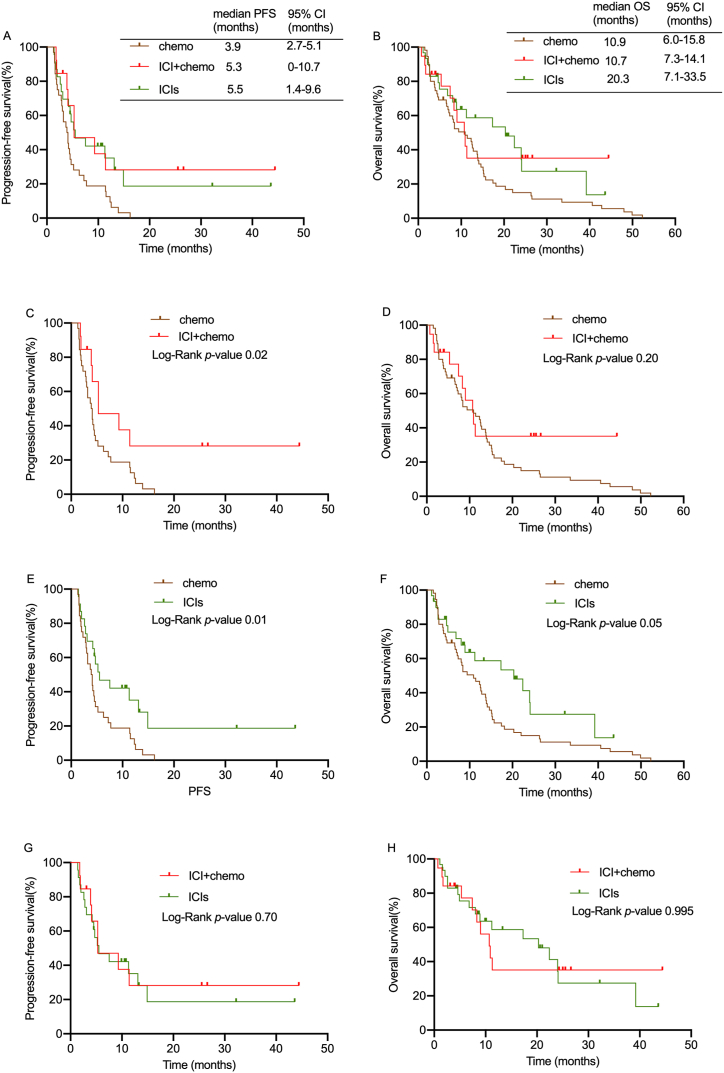
In total population, the ICIs group has the highest disease control rate (DCR 75%). There were no significant differences in progression-free survival (PFS) and overall survival (OS) among older patients between ICI + chemo and ICIs groups (PFS: 5.3 months vs. 5.5 months, = 0.70, OS: 10.7 months vs. 20.3 months, 0.995). Meanwhile, we observed ICIs had a longer PFS and OS than chemo group (PFS: 3.9 months vs. 5.5 months, = 0.01, OS: 10.9 months vs. 20.3 months, 0.05). Subgroup analysis showed that patients with programmed death ligand-1 (PD-L1) ≥ 1% had a distinct longer trend toward OS in ICIs group compared to ICI + chemo group (22.4 months vs. 10.7 months, = 0.605), even though there was no significant difference. In terms of safety, ICIs was more tolerable and had a lower discontinuation rate than ICI + chemo group.
In the real world, ICI + chemo is more likely to be discontinued due to adverse effects and does not significantly improve patient survival compared with ICIs treatment in total population and subgroup. Therefore, ICI alone or ICIs plus other therapies, such as anti-angiogenesis drugs or other novel ICI (ICIs) could be recommended for older cases with PD-L1 positive NSCLC.
本研究旨在探讨免疫检查点抑制剂(ICIs)或联合化疗在老年患者中的疗效和安全性。
我们纳入了110例年龄≥75岁的非小细胞肺癌(NSCLC)老年患者,这些患者接受了单纯化疗(化疗组)、ICI联合化疗(ICI + 化疗组)、单纯ICI或ICI联合其他治疗,其中包括抗血管生成药物或其他新型ICI(ICIs)。评估了患者的特征、治疗反应、生存率和毒性。
在总体人群中,ICIs组的疾病控制率最高(疾病控制率为75%)。ICI + 化疗组和ICIs组的老年患者在无进展生存期(PFS)和总生存期(OS)方面无显著差异(PFS:5.3个月对5.5个月,P = 0.70;OS:10.7个月对20.3个月,P = 0.995)。同时,我们观察到ICIs组的PFS和OS比化疗组长(PFS:3.9个月对5.5个月,P = 0.01;OS:10.9个月对20.3个月,P = 0.05)。亚组分析显示,程序性死亡配体-1(PD-L1)≥1%的患者中,ICIs组的OS趋势明显长于ICI + 化疗组(22.4个月对10.7个月,P = 0.605),尽管无显著差异。在安全性方面,ICIs比ICI + 化疗组更具耐受性,停药率更低。
在现实世界中,ICI + 化疗因不良反应更易停药,与总体人群和亚组中的ICIs治疗相比,并未显著改善患者生存。因此,对于PD-L1阳性的NSCLC老年患者,可推荐单纯ICI或ICI联合其他治疗,如抗血管生成药物或其他新型ICI(ICIs)。