Feng Yong, Chen Ning, Dai Bing, Shang Yunxiao
Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang, China.
Front Pediatr. 2024 Feb 8;12:1341188. doi: 10.3389/fped.2024.1341188. eCollection 2024.
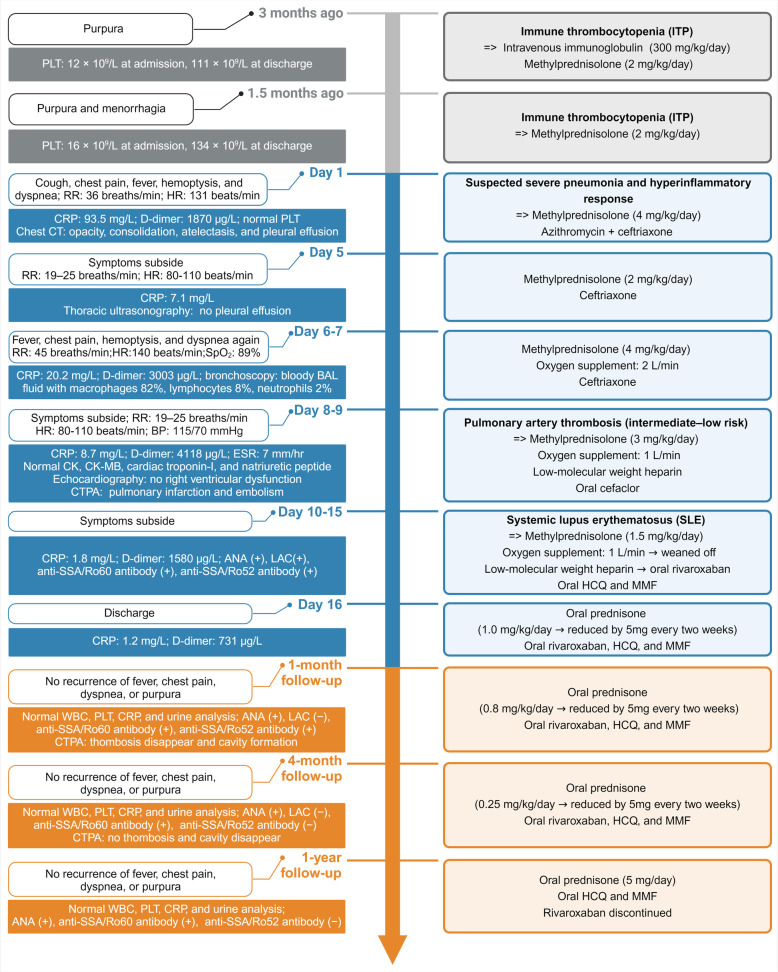
pulmonary artery thrombosis (ISPAT) is a relatively rare but potentially life-threatening complication of systemic lupus erythematosus (SLE) in children. We report the case of a 12-year-old girl who presented with fever, chest pain, and dyspnea. Immune thrombocytopenia was identified due to purpura and menorrhagia 3 months before presentation with a lowest platelet count of 12 × 10/L. The sudden onset of fever, chest pain, and dyspnea were misdiagnosed as hyperinflammatory responses caused by pneumonia; these symptoms ameliorated with glucocorticoid and antibiotic treatment. The reappearance of symptoms after dose reduction of glucocorticoids and the observation of bloody bronchoalveolar lavage fluid necessitated further evaluation. Pulmonary artery thrombosis/embolism was identified using computed tomography pulmonary angiography and high D-dimer quantitative level of 4,118 μg/L (normal <252 μg/L). Ultrasonography of the deep and superficial veins of both lower limbs and renal veins revealed no thrombosis, suggesting the diagnosis of ISPAT. Further etiological evaluation revealed positive antinuclear antibodies, lupus anticoagulant, and anti-SSA antibodies, confirming SLE. Repeated normal urine analysis indicated that lupus nephritis was unlikely. Further, the negative anticardiolipin and anti-β glycoprotein antibodies and temporary positive lupus anticoagulant suggested that antiphospholipid syndrome was unlikely. The patient received anticoagulants, glucocorticoids, hydroxychloroquine, and mycophenolate therapy. Her symptoms gradually improved, and she was discharged. At the 1-month follow-up, the thrombosis had resolved. During the 1-year follow-up, her condition remained well without SLE relapse. Our experience with this case emphasizes searching for SLE in the case of ISPAT and pulmonary hemorrhages. ISPAT can occur in children with SLE and may be caused by hyperinflammatory response during SLE flare.
儿童肺动脉血栓形成(ISPAT)是系统性红斑狼疮(SLE)相对罕见但可能危及生命的并发症。我们报告了一名12岁女孩的病例,她出现发热、胸痛和呼吸困难。在出现症状前3个月,因紫癜和月经过多确诊免疫性血小板减少症,最低血小板计数为12×10⁹/L。发热、胸痛和呼吸困难的突然发作被误诊为由肺炎引起的高炎症反应;这些症状经糖皮质激素和抗生素治疗后有所改善。糖皮质激素减量后症状再次出现,且观察到支气管肺泡灌洗呈血性,因此需要进一步评估。通过计算机断层扫描肺动脉造影和高D-二聚体定量水平4118μg/L(正常<252μg/L)确定为肺动脉血栓形成/栓塞。双下肢深浅静脉及肾静脉超声检查未发现血栓,提示诊断为ISPAT。进一步的病因评估显示抗核抗体、狼疮抗凝物和抗SSA抗体阳性,确诊为SLE。多次尿常规分析正常表明不太可能患有狼疮性肾炎。此外,抗心磷脂和抗β糖蛋白抗体阴性以及狼疮抗凝物暂时阳性表明抗磷脂综合征不太可能。患者接受了抗凝剂、糖皮质激素、羟氯喹和霉酚酸酯治疗。她的症状逐渐改善并出院。在1个月的随访中,血栓已溶解。在1年的随访中,她的病情保持良好,无SLE复发。我们对该病例的经验强调在ISPAT和肺出血病例中寻找SLE。ISPAT可发生于SLE患儿,可能由SLE发作期间的高炎症反应引起。