Kawuma Samuel, Katwesigye Rogers, Walusaga Happy, Akatukunda Praise, Nangendo Joan, Kabugo Charles, Kamya Moses R, Semitala Fred C
Makerere University Joint AIDS Program.
Infectious Diseases Research Collaboration.
Res Sq. 2024 Feb 9:rs.3.rs-3914483. doi: 10.21203/rs.3.rs-3914483/v1.
Female sex workers (FSWs) have the highest HIV prevalence in Uganda. Pre exposure prophylaxis (PrEP) has been recommended as part of the HIV combination prevention strategy, with improved patient initiation, but continuation on the service is low. We evaluated PrEP continuation among FSWs and explored potential determinants of PrEP continuation within a public referral hospital in Urban Uganda.
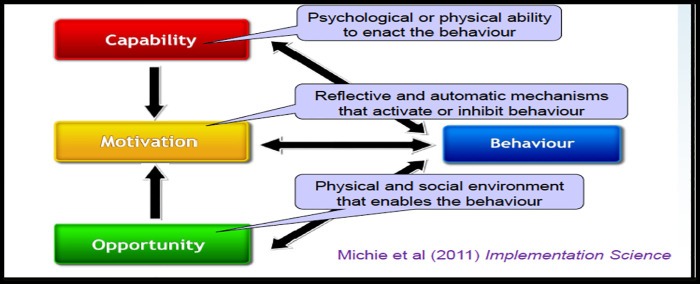
An explanatory sequential mixed method study was conducted at Kiruddu National referral hospital in Uganda. Secondary data on social demographic characteristics and follow up outcomes of at least one year was collected for all FSWs who were initiated PrEP between May 2020 and April 2021.We used Kaplan-Meier survival analysis to evaluate continuation on PrEP from time of initiation and follow-up period. The capability, opportunity, and motivation to change behaviour model was used to explore perspectives and practices of FSWs (n = 24) and health care providers (n = 8) on continuation on PrEP among FSWs, using semi structured interviews. The qualitative data was deductively coded and analyzed thematically, categorizing the themes related to PrEP continuation as facilitators and barriers.
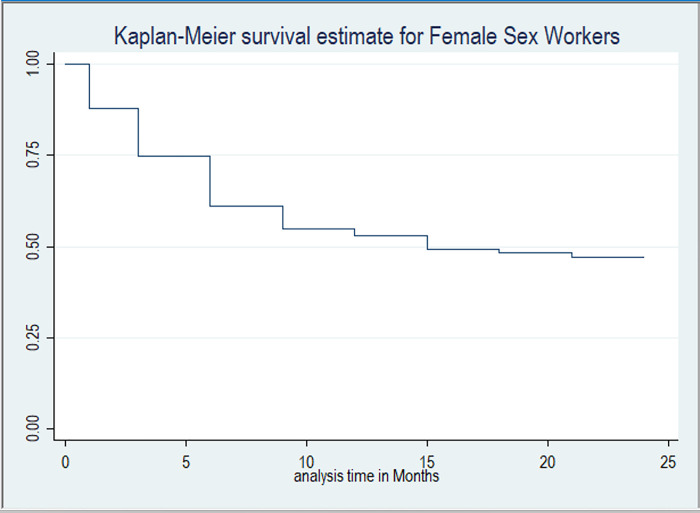
Of the 292 FSWs initiated on PrEP during this period, 101 (34.6) % were active on PrEP, 137 (46.9%) were lost to follow-up, 45 (15.4%) were no longer eligible to continue PrEP, eight (2.7%) were transferred out and one (0.3%) had died. Median survival time on PrEP was 15 months (Interquartile range IQR, 3-21). The continuation rates on PrEP at six (6) and 12 months were, 61.1% and 53.1%, respectively. Facilitators of PrEP continuation included awareness of risk associated with sex work, integration of PrEP with other HIV prevention services, presence of PrEP Peer support and use of Drop-in centers. The barriers included low community awareness about PrEP, high mobility of sex workers, substance abuse, and the unfavorable daytime clinic schedules.
Continuation on PrEP remains low among FSWs. Interventions for PrEP continuation should address barriers such as low community awareness on PrEP, substance abuse and restrictive health facility policies for scale of the PrEP program among FSWs in Uganda. Integration of PrEP with other services and scale up of community PrEP delivery structures may improve its continuation.
在乌干达,女性性工作者的艾滋病毒感染率最高。暴露前预防(PrEP)已被推荐作为艾滋病毒联合预防策略的一部分,患者开始接受该预防措施的情况有所改善,但继续接受该服务的比例较低。我们评估了乌干达城市一家公共转诊医院内女性性工作者继续接受PrEP的情况,并探讨了PrEP继续接受情况的潜在决定因素。
在乌干达的基鲁杜国家转诊医院进行了一项解释性序贯混合方法研究。收集了2020年5月至2021年4月期间开始接受PrEP的所有女性性工作者的社会人口特征和至少一年随访结果的二手数据。我们使用Kaplan-Meier生存分析来评估从开始接受PrEP到随访期的继续接受情况。使用改变行为的能力、机会和动机模型,通过半结构化访谈探讨女性性工作者(n = 24)和医疗服务提供者(n = 8)对女性性工作者继续接受PrEP的看法和做法。对定性数据进行演绎编码并进行主题分析,将与PrEP继续接受相关的主题分为促进因素和障碍。
在此期间开始接受PrEP的292名女性性工作者中,101名(34.6%)仍在积极接受PrEP,137名(46.9%)失访,45名(15.4%)不再符合继续接受PrEP的条件,8名(2.7%)转出,1名(0.3%)死亡。PrEP的中位生存时间为15个月(四分位间距IQR,3 - 21)。6个月和12个月时PrEP的继续接受率分别为61.1%和53.1%。PrEP继续接受的促进因素包括对性工作相关风险的认识、PrEP与其他艾滋病毒预防服务的整合、PrEP同伴支持的存在以及使用救助中心。障碍包括社区对PrEP的认识不足、性工作者的高流动性、药物滥用以及日间门诊时间表不利。
女性性工作者中继续接受PrEP的比例仍然较低。针对PrEP继续接受情况的干预措施应解决诸如社区对PrEP认识不足、药物滥用以及乌干达女性性工作者PrEP项目规模方面卫生设施政策限制等障碍。将PrEP与其他服务整合以及扩大社区PrEP提供结构可能会提高其继续接受率。