Center for Respiratory and Pulmonary Vascular Diseases, National Center for Cardiovascular Diseases, National Clinical Research Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Fuwai Hospital, Beijing, China.
Department of ICU, Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu, China.
Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241232521. doi: 10.1177/17534666241232521.
Balloon pulmonary angioplasty (BPA) is typically performed in a sequential manner.
This study aimed to determine the lowest frequency of BPA for patients who could not reach treatment goals in a short period.
Retrospective cohort.
We retrospectively enrolled 186 BPA-treated patients diagnosed with chronic thromboembolic pulmonary hypertension. According to the accumulative number of performed BPA sessions or treated pulmonary vessels or the ratio of the number of treated pulmonary vessels/the number of baseline lesions (T/P) prior to the initial occurrence of clinical outcome or censored date, we divided patients into different groups. The principal outcome was clinical worsening.
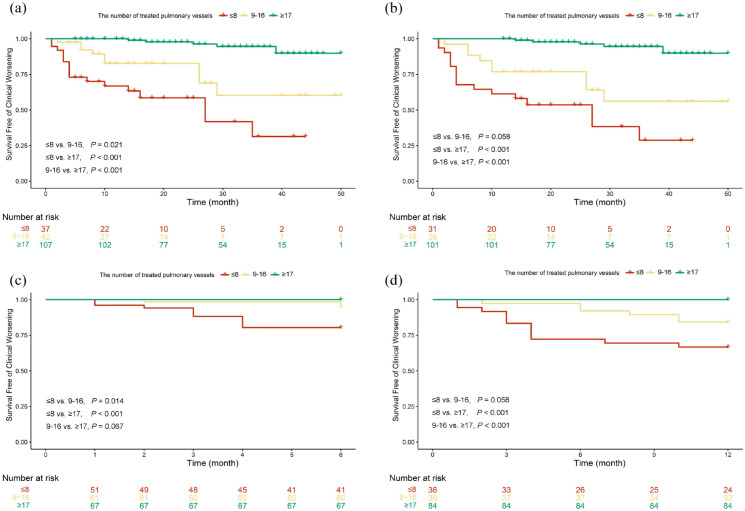
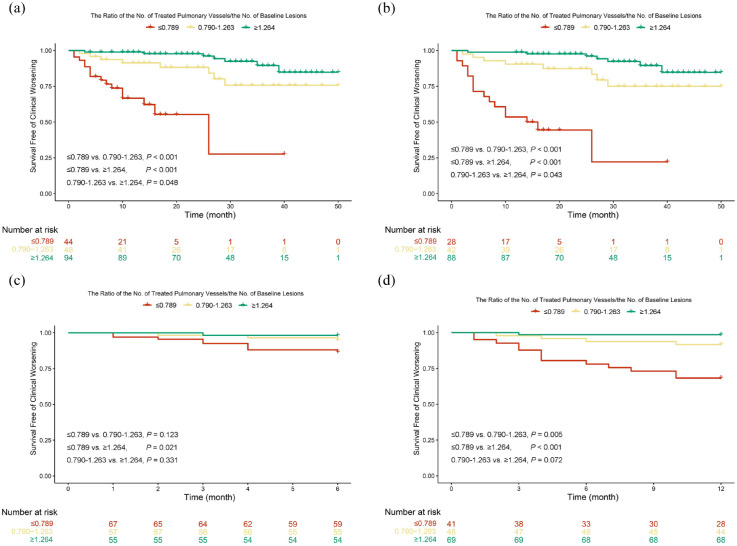
After stratifying patients by the number of performed BPA sessions, most baseline parameters were comparable among groups. During follow-up, 31 (16.7%) of 186 patients experienced clinical worsening. The 6-month cumulative clinical worsening-free survival rates of ⩾2 performed sessions group were significantly higher than that of 1 performed session group. The 12-month cumulative rates of clinical worsening-free survival exhibited a declining pattern in the subsequent sequence: ⩾3, 2, and 1 performed BPA sessions, and this trend persisted when follow-up time exceeded 12 months. The 6-, 12-, and 24-month cumulative clinical worsening-free survival rates were comparable between patients with 3 and ⩾4 performed BPA sessions. Similar results were also observed when stratifying patients by the accumulative number of treated pulmonary vessels (⩽8, 9-16, ⩾17) and T/P (⩽0.789, 0.790-1.263, ⩾1.264).
To achieve optimal short-term outcomes, patients might need to undergo ⩾2 BPA sessions or have ⩾9 pulmonary vessels treated or have T/P ⩾0.790 within 6 months, and undergo ⩾3 BPA sessions or have ⩾17 pulmonary vessels treated or have T/P ⩾1.264 within 12 months.
球囊肺血管成形术(BPA)通常是按顺序进行的。
本研究旨在确定在短时间内无法达到治疗目标的患者进行 BPA 的最低频率。
回顾性队列研究。
我们回顾性纳入了 186 例接受慢性血栓栓塞性肺动脉高压治疗的 BPA 患者。根据累积的 BPA 治疗次数、治疗的肺动脉数量或初始临床结果发生或截止日期前的治疗肺动脉数量/基线病变数量的比值(T/P),我们将患者分为不同的组。主要结局是临床恶化。
根据 BPA 治疗次数分层患者后,大多数基线参数在各组之间无差异。在随访期间,186 例患者中有 31 例(16.7%)发生了临床恶化。接受 ⩾2 次 BPA 治疗的患者 6 个月累积无临床恶化生存率明显高于接受 1 次 BPA 治疗的患者。12 个月无临床恶化生存率呈递减模式:接受 ⩾3、2 和 1 次 BPA 治疗的患者。当随访时间超过 12 个月时,这一趋势仍然存在。接受 3 次和 ⩾4 次 BPA 治疗的患者的 6、12 和 24 个月累积无临床恶化生存率无差异。按累积治疗的肺动脉数量(⩽8、9-16、⩾17)和 T/P(⩽0.789、0.790-1.263、⩾1.264)分层时也观察到类似的结果。
为了达到最佳的短期疗效,患者可能需要在 6 个月内接受 ⩾2 次 BPA 治疗或治疗 ⩾9 个肺动脉或 T/P ⩾0.790,或在 12 个月内接受 ⩾3 次 BPA 治疗或治疗 ⩾17 个肺动脉或 T/P ⩾1.264。