Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands.
Department of Clinical Science, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden.
Nephrol Dial Transplant. 2024 Sep 27;39(10):1672-1682. doi: 10.1093/ndt/gfae050.
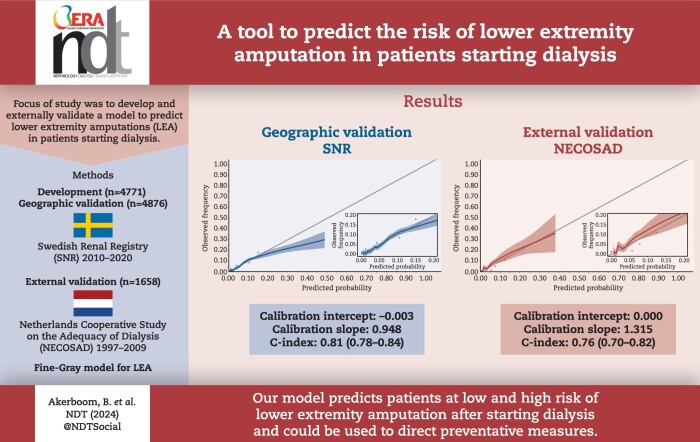
Non-traumatic lower extremity amputation (LEA) is a severe complication during dialysis. To inform decision-making for physicians, we developed a multivariable prediction model for LEA after starting dialysis.
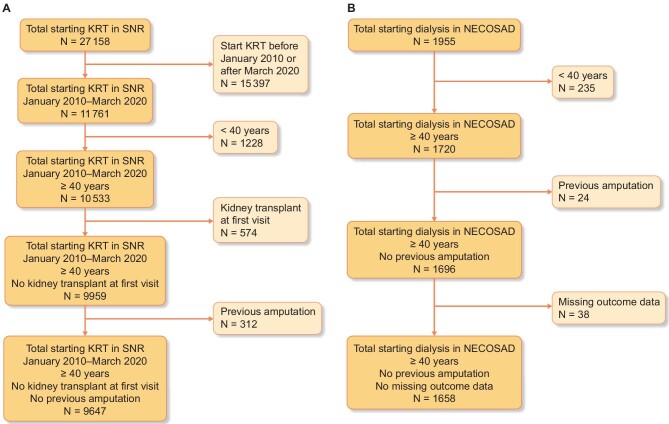
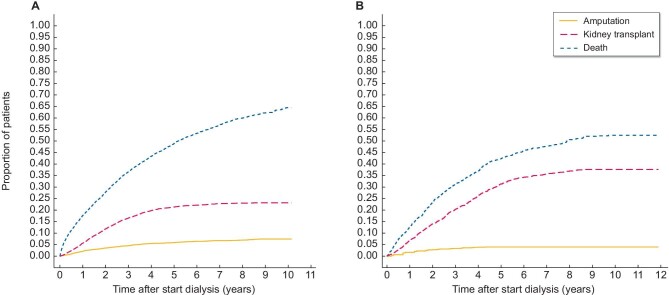
Data from the Swedish Renal Registry (SNR) between 2010 and 2020 were geographically split into a development and validation cohort. Data from Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD) between 1997 and 2009 were used for validation targeted at Dutch patients. Inclusion criteria were no previous LEA and kidney transplant and age ≥40 years at baseline. A Fine-Gray model was developed with LEA within 3 years after starting dialysis as the outcome of interest. Death and kidney transplant were treated as competing events. One coefficient, ordered by expected relevance, per 20 events was estimated. Performance was assessed with calibration and discrimination.
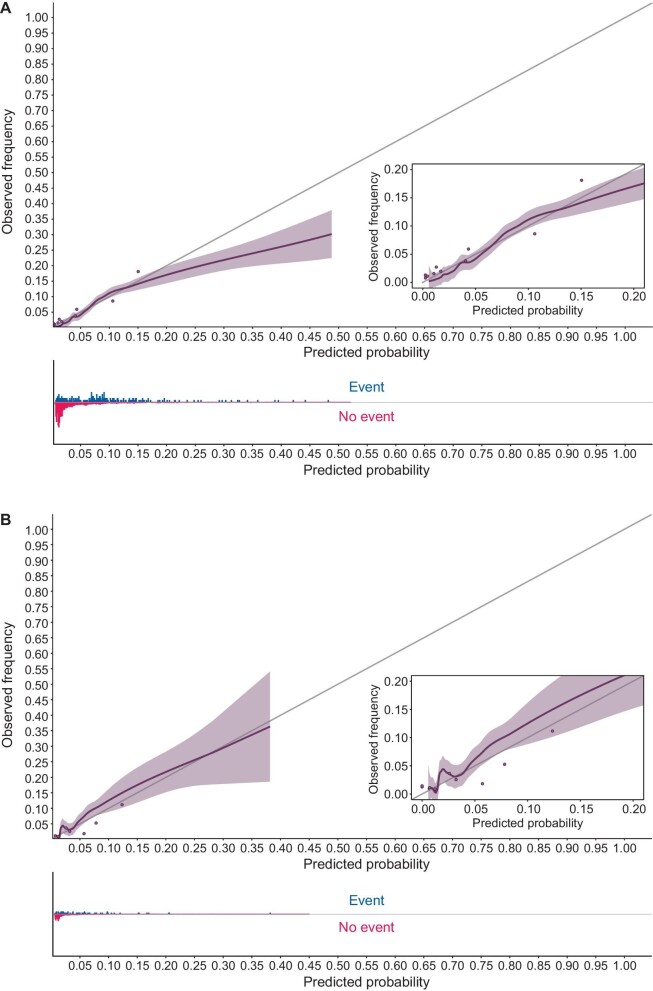
SNR was split into an urban development cohort with 4771 individuals experiencing 201 (4.8%) events and a rural validation cohort with 4.876 individuals experiencing 155 (3.2%) events. NECOSAD contained 1658 individuals experiencing 61 (3.7%) events. Ten predictors were included: female sex, age, diabetes mellitus, peripheral artery disease, cardiovascular disease, congestive heart failure, obesity, albumin, haemoglobin and diabetic retinopathy. In SNR, calibration intercept and slope were -0.003 and 0.912, respectively. The C-index was estimated as 0.813 (0.783-0.843). In NECOSAD, calibration intercept and slope were 0.001 and 1.142 respectively. The C-index was estimated as 0.760 (0.697-0.824). Calibration plots showed good calibration.
A newly developed model to predict LEA after starting dialysis showed good discriminatory performance and calibration. By identifying high-risk individuals this model could help select patients for preventive measures.
非外伤性下肢截肢(LEA)是透析期间的严重并发症。为了为医生提供决策依据,我们开发了一种透析后 LEA 的多变量预测模型。
2010 年至 2020 年期间,瑞典肾脏登记处(SNR)的数据在地理上分为开发和验证队列。1997 年至 2009 年期间荷兰合作透析充分性研究(NECOSAD)的数据用于针对荷兰患者的验证。纳入标准为基线时无先前的 LEA 和肾移植,年龄≥40 岁。使用 Fine-Gray 模型,以透析后 3 年内的 LEA 为感兴趣的结局。死亡和肾移植被视为竞争事件。每 20 个事件估计一个按预期相关性排序的系数。使用校准和区分度评估性能。
SNR 被分为一个城市开发队列,其中 4771 人经历了 201 次(4.8%)事件,一个农村验证队列,其中 4876 人经历了 155 次(3.2%)事件。NECOSAD 包含 1658 人经历了 61 次(3.7%)事件。纳入了 10 个预测因素:女性、年龄、糖尿病、外周动脉疾病、心血管疾病、充血性心力衰竭、肥胖、白蛋白、血红蛋白和糖尿病视网膜病变。在 SNR 中,校准截距和斜率分别为-0.003 和 0.912。C 指数估计为 0.813(0.783-0.843)。在 NECOSAD 中,校准截距和斜率分别为 0.001 和 1.142。C 指数估计为 0.760(0.697-0.824)。校准图显示了良好的校准。
一种新开发的预测透析后 LEA 的模型显示出良好的区分性能和校准。通过识别高风险个体,该模型可以帮助选择患者进行预防措施。