Department of Diagnostic and Interventional Neuroradiology, University Hospital Bern Inselspital, University of Bern, Bern, Switzerland.
Department of Neurology, University Hospital Frankfurt, Goethe University, Frankfurt am Main, Germany.
Eur J Neurol. 2024 Jun;31(6):e16256. doi: 10.1111/ene.16256. Epub 2024 Feb 26.
The value of intravenous thrombolysis (IVT) in eligible tandem lesion patients undergoing endovascular treatment (EVT) is unknown. We investigated treatment effect heterogeneity of EVT + IVT versus EVT-only in tandem lesion patients. Additional analyses were performed for patients undergoing emergent internal carotid artery (ICA) stenting.
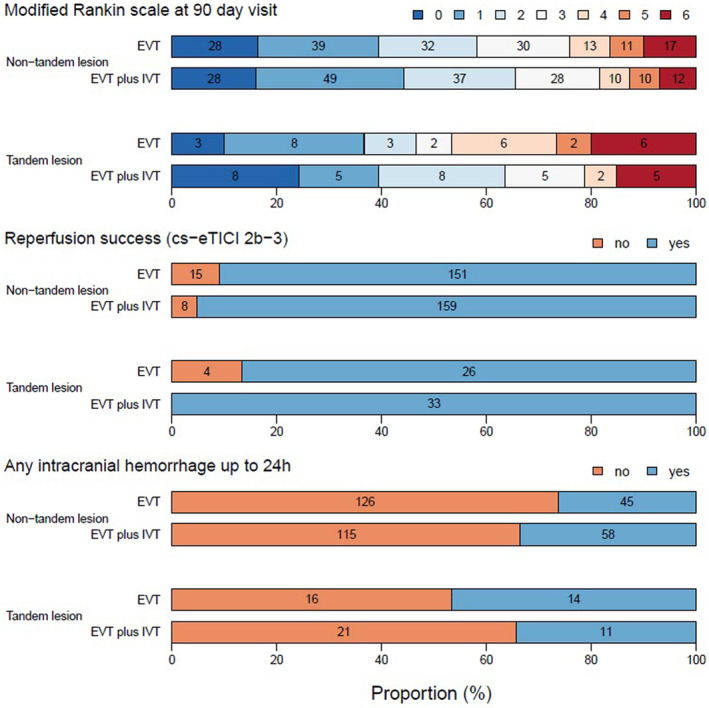
SWIFT DIRECT randomized IVT-eligible patients to either EVT + IVT or EVT-only. Primary outcome was 90-day functional independence (modified Rankin Scale score 0-2) after the index event. Secondary endpoints were reperfusion success, 24 h intracranial hemorrhage rate, and 90-day all-cause mortality. Interaction models were fitted for all predefined outcomes.
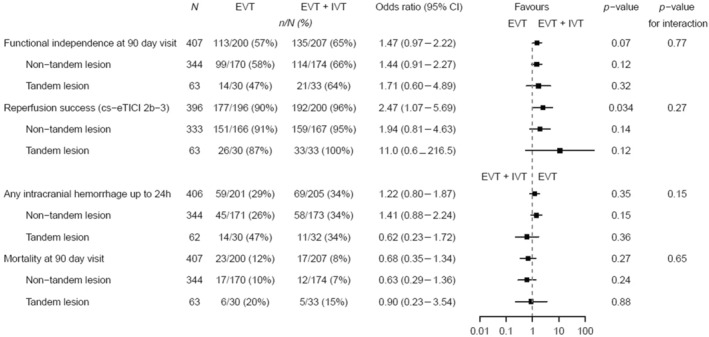
Among 408 included patients, 63 (15.4%) had a tandem lesion and 33 (52.4%) received IVT. In patients with tandem lesions, 20 had undergone emergent ICA stenting (EVT + IVT: 9/33, 27.3%; EVT: 11/30, 36.7%). Tandem lesion did not show treatment effect modification of IVT on rates of functional independence (tandem lesion EVT + IVT vs. EVT: 63.6% vs. 46.7%, non-tandem lesion EVT + IVT vs. EVT: 65.6% vs. 58.2%; p for interaction = 0.77). IVT also did not increase the risk of intracranial hemorrhage among tandem lesion patients (tandem lesion EVT + IVT vs. EVT: 34.4% vs. 46.7%, non-tandem lesion EVT + IVT vs. EVT: 33.5% vs. 26.3%; p for interaction = 0.15). No heterogeneity was noted for other endpoints (p for interaction > 0.05).
No treatment effect heterogeneity of EVT + IVT versus EVT-only was observed among tandem lesion patients. Administering IVT in patients with anticipated emergent ICA stenting seems safe, and the latter should not be a factor to consider when deciding to administer IVT before EVT.
在接受血管内治疗(EVT)的适合串联病变患者中,静脉溶栓(IVT)的价值尚不清楚。我们研究了 EVT+IVT 与 EVT 仅治疗在串联病变患者中的治疗效果异质性。对接受紧急颈内动脉(ICA)支架置入术的患者进行了额外的分析。
SWIFT DIRECT 将符合 IVT 条件的患者随机分配至 EVT+IVT 或 EVT 仅治疗组。主要终点为指数事件后 90 天的功能独立性(改良 Rankin 量表评分 0-2)。次要终点为再灌注成功、24 小时颅内出血率和 90 天全因死亡率。为所有预先设定的结局拟合了交互模型。
在纳入的 408 例患者中,63 例(15.4%)存在串联病变,33 例(52.4%)接受了 IVT。在存在串联病变的患者中,20 例接受了紧急 ICA 支架置入术(EVT+IVT:9/33,27.3%;EVT:11/30,36.7%)。串联病变并未改变 IVT 对功能独立性的治疗效果(串联病变 EVT+IVT 与 EVT:63.6%与 46.7%,非串联病变 EVT+IVT 与 EVT:65.6%与 58.2%;p 交互 = 0.77)。IVT 也未增加串联病变患者颅内出血的风险(串联病变 EVT+IVT 与 EVT:34.4%与 46.7%,非串联病变 EVT+IVT 与 EVT:33.5%与 26.3%;p 交互 = 0.15)。其他终点均未观察到异质性(p 交互 > 0.05)。
在串联病变患者中,EVT+IVT 与 EVT 仅治疗之间未观察到治疗效果的异质性。在预计需要紧急 ICA 支架置入术的患者中使用 IVT 似乎是安全的,在决定在 EVT 之前进行 IVT 时,后者不应成为考虑因素。