Marnat Gaultier, Sibon Igor, Bourcier Romain, Anadani Mohammad, Gariel Florent, Labreuche Julien, Kyheng Maeva, Mazighi Mikael, Dargazanli Cyril, Piotin Michel, Consoli Arturo, Blanc Raphaël, Anxionnat René, Audibert Gérard, Richard Sébastien, Lapergue Bertrand, Gory Benjamin
Department of Neuroradiology, University Hospital of Bordeaux, Bordeaux, France.
Department of Neurology, University Hospital of Bordeaux, Bordeaux, France.
J Stroke. 2021 Sep;23(3):411-419. doi: 10.5853/jos.2020.04889. Epub 2021 Sep 30.
Despite the widespread adoption of mechanical thrombectomy (MT) for the treatment of large vessel occlusion stroke (LVOS) in the anterior circulation, the optimal strategy for the treatment tandem occlusion related to cervical internal carotid artery (ICA) dissection is still debated. This individual patient pooled analysis investigated the safety and efficacy of prior intravenous thrombolysis (IVT) in anterior circulation tandem occlusion related to cervical ICA dissection treated with MT.
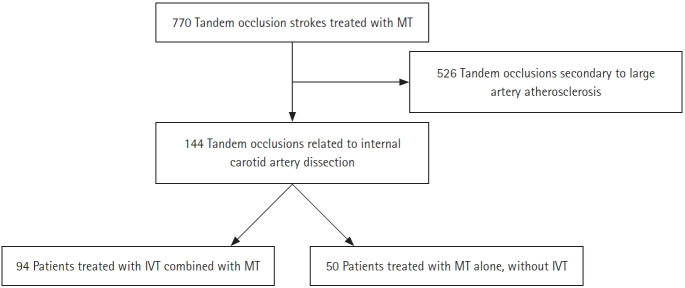
We performed a retrospective analysis of two merged prospective multicenter international real-world observational registries: Endovascular Treatment in Ischemic Stroke (ETIS) and Thrombectomy In TANdem occlusions (TITAN) registries. Data from MT performed in the treatment of tandem LVOS related to cervical ICA dissection between January 2012 and December 2019 at 24 comprehensive stroke centers were analyzed. The primary endpoint was a favorable outcome defined as 90-day modified Rankin Scale (mRS) score of 0-2.
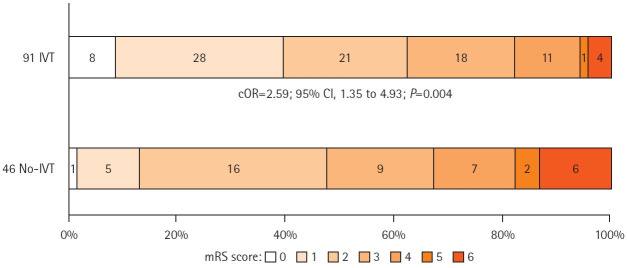
The study included 144 patients with tandem occlusion LVOS due to cervical ICA dissection, of whom 94 (65.3%) received IVT before MT. Prior IVT was significantly associated with a better clinical outcome considering the mRS shift analysis (common odds ratio, 2.59; 95% confidence interval [CI], 1.35 to 4.93; P=0.004 for a 1-point improvement) and excellent outcome (90-day mRS 0-1) (adjusted odds ratio [aOR], 4.23; 95% CI, 1.60 to 11.18). IVT was also associated with a higher rate of intracranial successful reperfusion (83.0% vs. 64.0%; aOR, 2.70; 95% CI, 1.21 to 6.03) and a lower rate of symptomatic intracranial hemorrhage (4.3% vs. 14.8%; aOR, 0.21; 95% CI, 0.05 to 0.80).
Prior IVT before MT for the treatment of tandem occlusion related to cervical ICA dissection was safe and associated with an improved 90-day functional outcome.
尽管机械取栓术(MT)已广泛应用于前循环大血管闭塞性卒中(LVOS)的治疗,但对于与颈内动脉(ICA)夹层相关的串联闭塞的最佳治疗策略仍存在争议。这项个体患者汇总分析研究了在接受MT治疗的与颈ICA夹层相关的前循环串联闭塞中,先行静脉溶栓(IVT)的安全性和有效性。
我们对两个合并的前瞻性多中心国际真实世界观察性注册研究进行了回顾性分析:缺血性卒中血管内治疗(ETIS)注册研究和串联闭塞取栓术(TITAN)注册研究。分析了2012年1月至2019年12月期间在24个综合卒中中心进行的与颈ICA夹层相关的串联LVOS治疗中MT的数据。主要终点是定义为90天改良Rankin量表(mRS)评分为0 - 2的良好结局。
该研究纳入了144例因颈ICA夹层导致串联闭塞LVOS的患者,其中94例(65.3%)在MT前接受了IVT。考虑到mRS移位分析,先行IVT与更好的临床结局显著相关(共同优势比,2.59;95%置信区间[CI],1.35至4.93;1分改善时P = 0.004)以及良好结局(90天mRS 0 - 1)(调整后优势比[aOR],4.23;95% CI,1.60至11.18)。IVT还与更高的颅内成功再灌注率(83.0%对64.0%;aOR,2.70;95% CI,1.21至6.03)和更低的有症状颅内出血率(4.3%对14.8%;aOR,0.21;95% CI,0.05至0.80)相关。
在MT前先行IVT治疗与颈ICA夹层相关的串联闭塞是安全的,并且与90天功能结局改善相关。