Department of Rheumatology and Clinical Immunology, Peking University First Hospital, Beijing, China.
Department of Geriatrics, Peking University First Hospital, Beijing, China.
RMD Open. 2024 Feb 27;10(1):e004016. doi: 10.1136/rmdopen-2023-004016.
Dysregulation of several inflammatory cytokines including tumour necrosis factor (TNF) in dementia patients has also been identified as a key factor in the pathogenesis of rheumatoid arthritis (RA). We aimed to investigate the association of disease-modifying antirheumatic drugs (DMARDs) therapy for RA with risk of incident dementia.
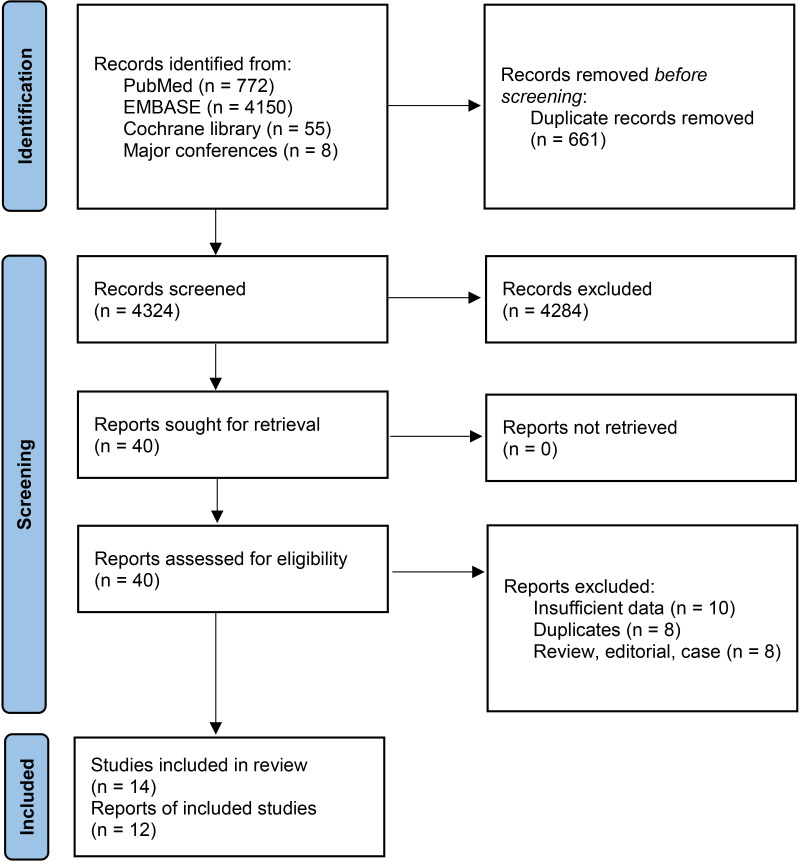
Electronic database searches of PubMed, EMBASE and Cochrane Library were performed. Observational studies that assessed the association of dementia with DMARDs in RA were included. Pooled risk ratios (RRs) with 95% CIs were used as summary statistic. The certainty of evidence was judged by using the Grading of Recommendations Assessment, Development and Evaluation system.
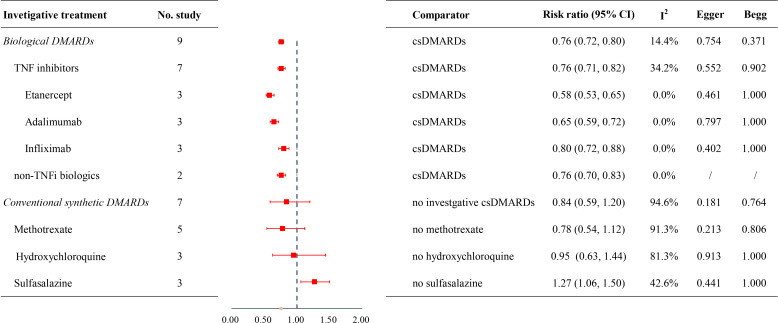
Overall, 14 studies involving 940 442 patients with RA were included. Pooled RR for developing dementia was 0.76 (95% CI 0.72 to 0.80) in patients taking biological DMARDs overall versus those taking conventional synthetic DMARDs, with 24% for TNF inhibitors (RR 0.76, 95% CI 0.71 to 0.82), 24% for non-TNF biologics (RR 0.76, 95% CI 0.70 to 0.83), separately. There was a significant subgroup effect among different types of TNF inhibitors (RR 0.58 [95%CI 0.53 to 0.65], 0.65 [95% CI 0.59 to 0.72], 0.80 [95% CI 0.72 to 0.88] for etanercept, adalimumab, infliximab, respectively; p value between groups=0.002). However, compared with non-users of DMARDs or investigative treatment, no significant effect on dementia incidence was observed in those receiving conventional synthetic DMARDs overall (RR 0.84, 95% CI 0.59 to 1.20), methotrexate (RR 0.78, 95% CI 0.54 to 1.12), hydroxychloroquine (RR 0.95, 95% CI 0.63 to 1.44), except for sulfasalazine (RR 1.27, 95% CI 1.06 to 1.50).
Biological DMARDs for RA are associated with decreased dementia risk, while protective effect is not observed in conventional synthetic DMARDs. Controlled clinical trials on TNF inhibitors are necessary to test their neuroprotective potentials.
在痴呆症患者中,几种炎症细胞因子(包括肿瘤坏死因子[TNF])的失调也被认为是类风湿关节炎(RA)发病机制中的一个关键因素。我们旨在研究改变病情的抗风湿药物(DMARDs)治疗 RA 与痴呆症发病风险的相关性。
对 PubMed、EMBASE 和 Cochrane 图书馆进行电子数据库检索。纳入了评估 DMARDs 治疗 RA 与痴呆症之间相关性的观察性研究。使用汇总风险比(RR)及其 95%置信区间(CI)作为汇总统计量。使用推荐评估、制定和评估系统(Grading of Recommendations Assessment, Development and Evaluation,GRADE)来评估证据的确定性。
总体而言,纳入了 14 项研究,共涉及 940442 例 RA 患者。与使用传统合成 DMARDs 的患者相比,使用生物 DMARDs 的患者发生痴呆的 RR 为 0.76(95%CI 0.72 至 0.80),其中 TNF 抑制剂的 RR 为 24%(RR 0.76,95%CI 0.71 至 0.82),非 TNF 生物制剂的 RR 为 24%(RR 0.76,95%CI 0.70 至 0.83)。不同类型的 TNF 抑制剂之间存在显著的亚组效应(依那西普的 RR 0.58 [95%CI 0.53 至 0.65]、阿达木单抗的 RR 0.65 [95%CI 0.59 至 0.72]、英夫利昔单抗的 RR 0.80 [95%CI 0.72 至 0.88];组间 p 值=0.002)。然而,与不使用 DMARDs 或研究性治疗相比,接受传统合成 DMARDs 治疗的患者(RR 0.84,95%CI 0.59 至 1.20)、甲氨蝶呤(RR 0.78,95%CI 0.54 至 1.12)、羟氯喹(RR 0.95,95%CI 0.63 至 1.44),包括柳氮磺胺吡啶(RR 1.27,95%CI 1.06 至 1.50),痴呆症发病风险未见显著影响。
RA 的生物 DMARDs 与痴呆风险降低相关,而传统合成 DMARDs 则无此保护作用。有必要进行针对 TNF 抑制剂的对照临床试验,以检验其神经保护潜力。