Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts.
Clinical and Translational Neuroscience Section, Laboratory of Behavioral Neuroscience, National Institute on Aging, Baltimore, Maryland.
JAMA Netw Open. 2022 Apr 1;5(4):e226567. doi: 10.1001/jamanetworkopen.2022.6567.
Cytokine signaling, including tumor necrosis factor (TNF) and interleukin (IL)-6, through the Janus-kinase (JAK)-signal transducer and activator of transcription pathway, was hypothesized to attenuate the risk of Alzheimer disease and related dementia (ADRD) in the Drug Repurposing for Effective Alzheimer Medicines (DREAM) initiative based on multiomics phenotyping.
To evaluate the association between treatment with tofacitinib, tocilizumab, or TNF inhibitors compared with abatacept and risk of incident ADRD.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study was conducted among US Medicare fee-for-service patients with rheumatoid arthritis aged 65 years and older from 2007 to 2017. Patients were categorized into 3 cohorts based on initiation of tofacitinib (a JAK inhibitor), tocilizumab (an IL-6 inhibitor), or TNF inhibitors compared with a common comparator abatacept (a T-cell activation inhibitor). Analyses were conducted from August 2020 to August 2021.
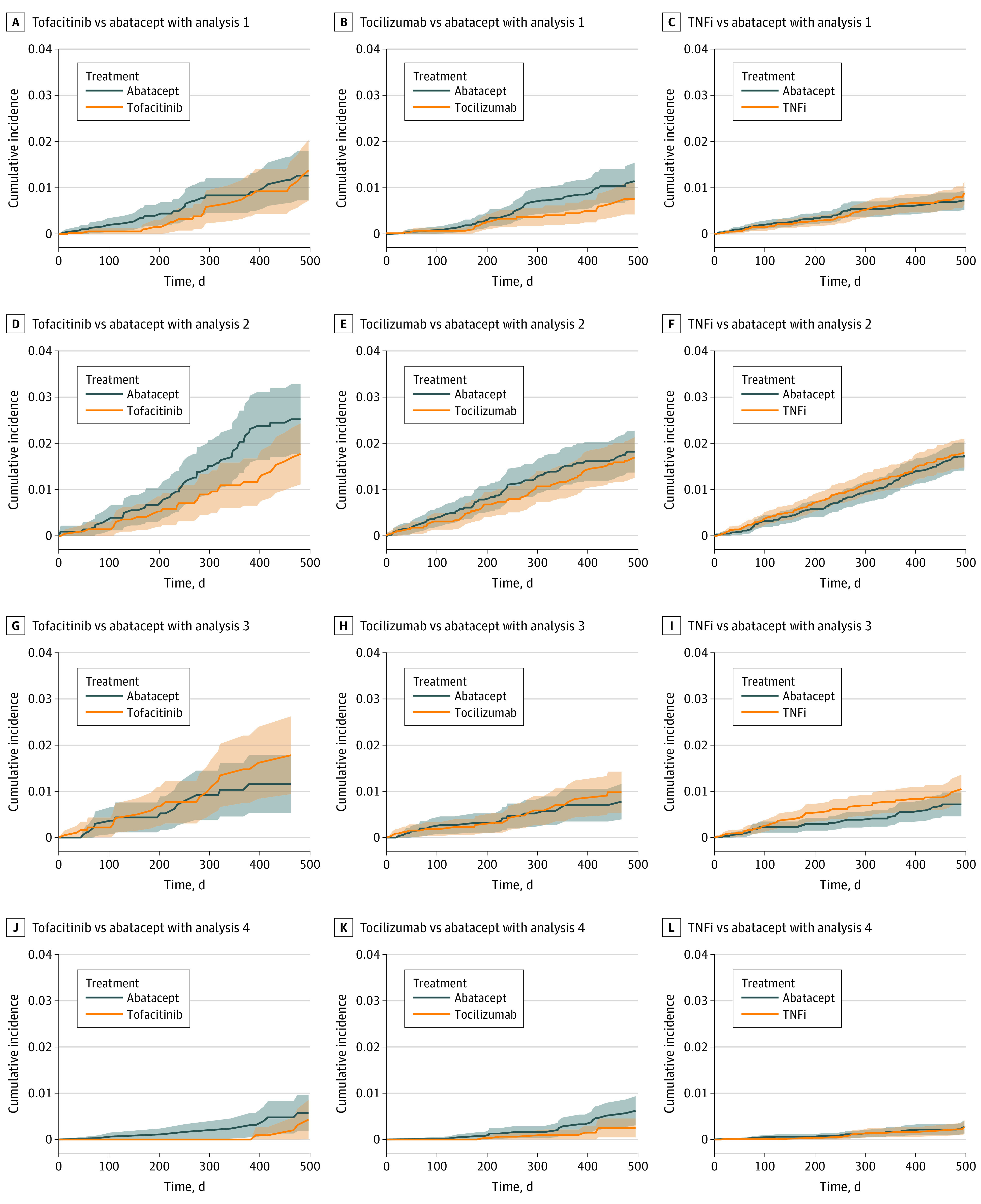
The main outcome was onset of ADRD based on diagnosis codes evaluated in 4 alternative analysis schemes: (1) an as-treated follow-up approach, (2) an as-started follow-up approach incorporating a 6-month induction period, (3) incorporating a 6-month symptom to diagnosis period to account for misclassification of ADRD onset, and (4) identifying ADRD through symptomatic prescriptions and diagnosis codes. Hazard ratios (HRs) with 95% CIs were calculated from Cox proportional hazard regression after adjustment for 79 preexposure characteristics through propensity score matching.
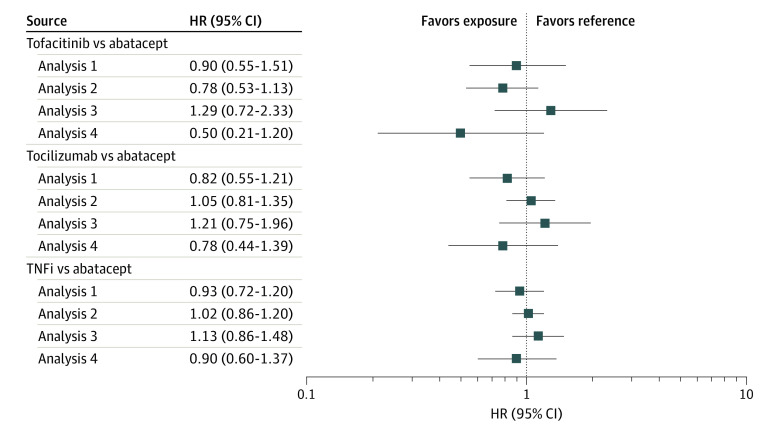
After 1:1 propensity score matching to patients using abatacept, a total of 22 569 propensity score-matched patient pairs, including 4224 tofacitinib pairs (mean [SD] age 72.19 [5.65] years; 6945 [82.2%] women), 6369 tocilizumab pairs (mean [SD] age 72.01 [5.46] years; 10 105 [79.4%] women), and 11 976 TNF inhibitor pairs (mean [SD] age 72.67 [5.91] years; 19 710 [82.3%] women), were assessed. Incidence rates of ADRD varied from 2 to 18 per 1000 person-years across analyses schemes. There were no statistically significant associations of ADRD with tofacitinib (analysis 1: HR, 0.90 [95% CI, 0.55-1.51]; analysis 2: HR, 0.78 [95% CI, 0.53-1.13]; analysis 3: HR, 1.29 [95% CI, 0.72-2.33]; analysis 4: HR, 0.50 [95% CI, 0.21-1.20]), tocilizumab (analysis 1: HR, 0.82 [95% CI, 0.55-1.21]; analysis 2: HR, 1.05 [95% CI, 0.81-1.35]; analysis 3: HR, 1.21 [95% CI, 0.75-1.96]; analysis 4: HR, 0.78 [95% CI, 0.44-1.39]), or TNF inhibitors (analysis 1: HR, 0.93 [95% CI, 0.72-1.20]; analysis 2: HR, 1.02 [95% CI, 0.86-1.20]; analysis 3: HR, 1.13 [95% CI, 0.86-1.48]; analysis 4: 0.90 [95% CI, 0.60-1.37]) compared with abatacept. Results from prespecified subgroup analysis by age, sex, and baseline cardiovascular disease were consistent except in patients with cardiovascular disease, for whom there was a potentially lower risk of ADRD with TNF inhibitors vs abatacept, but only in analyses 2 and 4 (analysis 1: HR, 0.76 [95% CI, 0.50-1.16]; analysis 2: HR, 0.74 [95% CI, 0.56-0.99]; analysis 3: HR, 1.03 [95% CI, 0.65-1.61]; analysis 4: HR, 0.45 [95% CI, 0.21-0.98]).
This cohort study did not find any association of risk of ADRD in patients treated with tofacitinib, tocilizumab, or TNF inhibitors compared with abatacept.
重要性:基于多组学表型的 Drug Repurposing for Effective Alzheimer Medicines(DREAM)计划推测,肿瘤坏死因子(TNF)和白细胞介素(IL)-6 等细胞因子信号通过 Janus-激酶(JAK)-信号转导和转录激活物(STAT)通路,可能会降低阿尔茨海默病和相关痴呆(ADRD)的风险。
目的:评估与阿巴西普相比,托法替布、托珠单抗或 TNF 抑制剂治疗与 ADRD 发病风险的关联。
设计、地点和参与者:本队列研究纳入了 2007 年至 2017 年期间美国医疗保险按服务收费计划中年龄在 65 岁及以上的类风湿关节炎患者。根据托法替布(一种 JAK 抑制剂)、托珠单抗(一种 IL-6 抑制剂)或 TNF 抑制剂与常见对照药物阿巴西普(一种 T 细胞激活抑制剂)的起始使用情况,将患者分为 3 个队列。分析于 2020 年 8 月至 2021 年 8 月进行。
主要结局和测量:主要结局是通过在 4 种替代分析方案中评估的 ADRD 发病情况:(1)基于治疗的随访方法,(2)包含 6 个月诱导期的起始随访方法,(3)包含 6 个月症状到诊断期以说明 ADRD 发病的误诊,(4)通过症状性处方和诊断代码识别 ADRD。采用 Cox 比例风险回归模型,在通过倾向评分匹配调整 79 个暴露前特征后,计算危险比(HR)及其 95%置信区间。
结果:在使用阿巴西普的患者中进行 1:1 的倾向评分匹配后,共有 22569 对经倾向评分匹配的患者,包括 4224 对托法替布(平均[SD]年龄 72.19[5.65]岁;6945[82.2%]女性)、6369 对托珠单抗(平均[SD]年龄 72.01[5.46]岁;10105[79.4%]女性)和 11976 对 TNF 抑制剂(平均[SD]年龄 72.67[5.91]岁;19710[82.3%]女性),评估了 ADRD 的发病风险。在不同的分析方案中,ADRD 的发生率在每 1000 人年 2 至 18 例之间。托法替布(分析 1:HR,0.90[95%CI,0.55-1.51];分析 2:HR,0.78[95%CI,0.53-1.13];分析 3:HR,1.29[95%CI,0.72-2.33];分析 4:HR,0.50[95%CI,0.21-1.20])、托珠单抗(分析 1:HR,0.82[95%CI,0.55-1.21];分析 2:HR,1.05[95%CI,0.81-1.35];分析 3:HR,1.21[95%CI,0.75-1.96];分析 4:HR,0.78[95%CI,0.44-1.39])或 TNF 抑制剂(分析 1:HR,0.93[95%CI,0.72-1.20];分析 2:HR,1.02[95%CI,0.86-1.20];分析 3:HR,1.13[95%CI,0.86-1.48];分析 4:HR,0.90[95%CI,0.60-1.37])与阿巴西普相比,ADRD 的发病风险没有显著差异。根据年龄、性别和基线心血管疾病的预先指定亚组分析结果一致,但在心血管疾病患者中,与阿巴西普相比,TNF 抑制剂可能会降低 ADRD 的风险,但仅在分析 2 和 4 中(分析 1:HR,0.76[95%CI,0.50-1.16];分析 2:HR,0.74[95%CI,0.56-0.99];分析 3:HR,1.03[95%CI,0.65-1.61];分析 4:HR,0.45[95%CI,0.21-0.98])。
结论和相关性:本队列研究未发现与阿巴西普相比,托法替布、托珠单抗或 TNF 抑制剂治疗与 ADRD 风险增加相关。