Division of Neurosurgery, Department of Surgery, National University Health System, Singapore, Singapore.
Department of Neurosurgery, King's College Hospital, London, UK.
Neurosurg Rev. 2024 Mar 1;47(1):100. doi: 10.1007/s10143-024-02325-z.
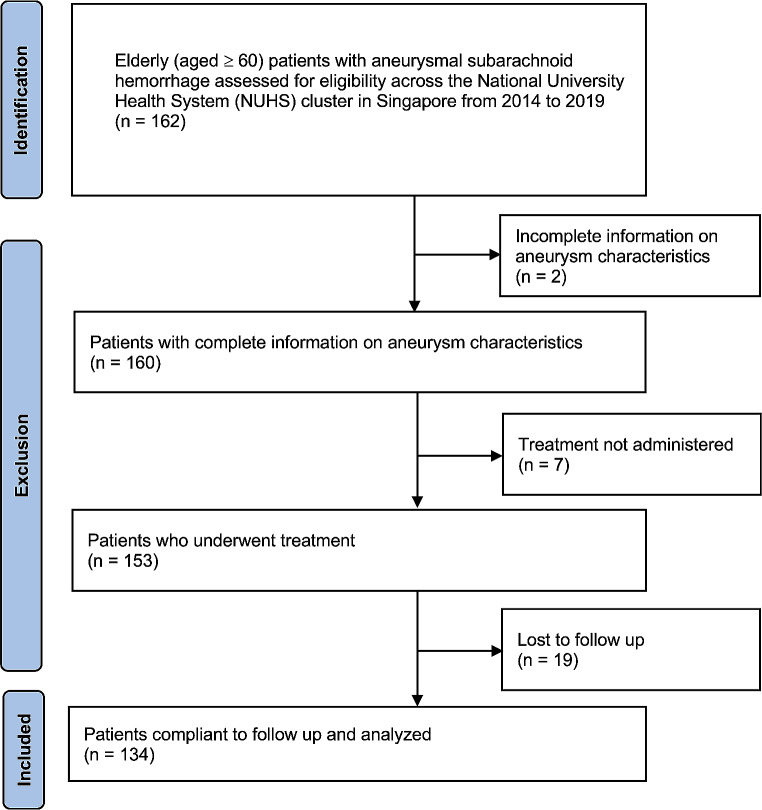
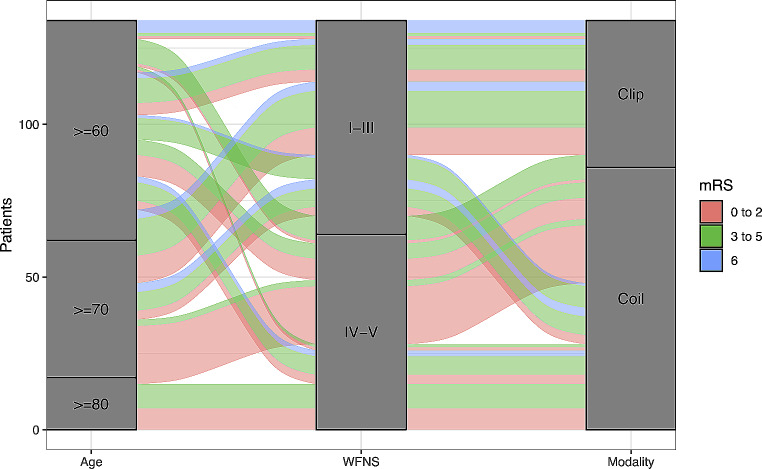
The comparability of endovascular coiling over neurosurgical clipping has not been firmly established in elderly patients with aneurysmal subarachnoid haemorrhage (aSAH). Data were obtained from all patients with aSAH aged ≥60 across three tertiary hospitals in Singapore from 2014 to 2019. Outcome measures included modified Rankin Scale (mRS) score at 3 and at 6 months, and in-hospital mortality. Of the 134 patients analyzed, 84 (62.7%) underwent coiling and 50 (37.3%) underwent clipping. The endovascular group showed a higher incidence of good mRS score 0-2 at 3 months (OR = 2.45 [95%CI:1.16-5.20];p = 0.018), and a lower incidence of in-hospital mortality (OR = 0.31 [95%CI:0.10-0.91];p = 0.026). There were no significant difference between the two treatment groups in terms of good mRS score at 6 months (OR = 1.98 [95%CI:0.97-4.04];p = 0.060). There were no significant differences in the incidence of complications, such as aneurysm rebleed, delayed hydrocephalus, delayed ischemic neurological deficit and venous thromboembolism between the two treatment groups. However, fewer patients in the coiling group developed large infarcts requiring decompressive craniectomy (OR = 0.32 [95%CI:0.12-0.90];p = 0.025). Age, admission WFNS score I-III, and coiling were independent predictors of good functional outcomes at 3 months. Only age and admission WFNS score I-III remained significant predictors of good functional outcomes at 6 months. Endovascular coiling, compared with neurosurgical clipping, is associated with significantly better short term outcomes in carefully selected elderly patients with aSAH. Maximal intervention is recommended for aSAH in the young elderly age group and those with favorable WFNS scores.
在老年颅内动脉瘤性蛛网膜下腔出血(aSAH)患者中,血管内介入治疗(弹簧圈栓塞)与开颅夹闭手术的疗效尚不确定。该研究数据来自新加坡三家三级医院 2014 年至 2019 年期间所有年龄≥60 岁的 aSAH 患者。结局指标包括改良 Rankin 量表(mRS)评分 3 个月和 6 个月,以及住院期间死亡率。在分析的 134 例患者中,84 例(62.7%)接受了弹簧圈栓塞治疗,50 例(37.3%)接受了开颅夹闭手术。血管内介入组在 3 个月时 mRS 评分 0-2 的比例更高(OR=2.45[95%CI:1.16-5.20];p=0.018),住院期间死亡率更低(OR=0.31[95%CI:0.10-0.91];p=0.026)。两组患者 6 个月时 mRS 评分良好的比例(OR=1.98[95%CI:0.97-4.04];p=0.060)无显著差异。两组患者的并发症发生率(如动脉瘤再出血、迟发性脑积水、迟发性缺血性神经功能缺损和静脉血栓栓塞)无显著差异。然而,弹簧圈组中需要去骨瓣减压术的大面积梗死的患者较少(OR=0.32[95%CI:0.12-0.90];p=0.025)。年龄、入院时 WFNS 评分 I-III 级和介入治疗是 3 个月时良好功能结局的独立预测因素。只有年龄和入院时 WFNS 评分 I-III 级是 6 个月时良好功能结局的独立预测因素。与开颅夹闭手术相比,血管内介入治疗与精心选择的老年 aSAH 患者的短期结局显著改善相关。对于年轻老年和 WFNS 评分有利的患者,建议最大程度地干预 aSAH。