Esson Gavin, Logan Ian, Wood Katrina, Browning Andrew C, Sayer John A
Renal Services, The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK.
Histopathology Department, The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, NE1 4LP UK.
J Rare Dis (Berlin). 2024;3(1):7. doi: 10.1007/s44162-024-00031-4. Epub 2024 Mar 1.
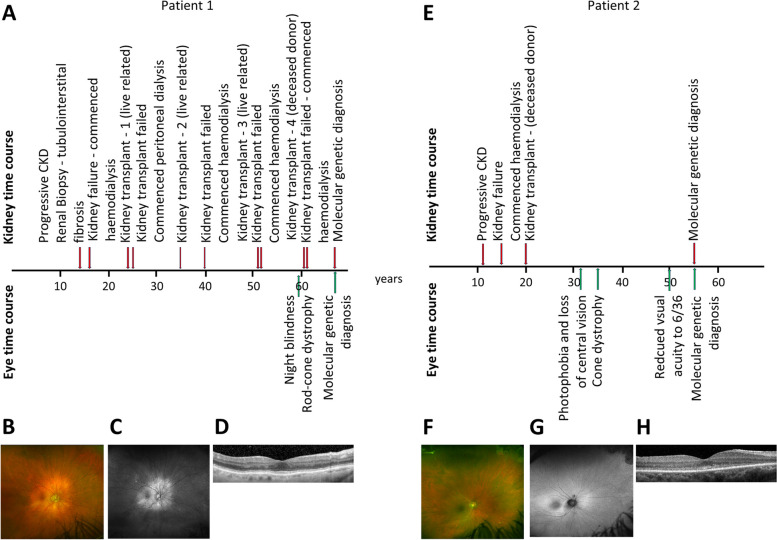
A precise diagnosis in medicine allows appropriate disease-specific management. Kidney failure of unknown aetiology remains a frequent diagnostic label within the haemodialysis unit and kidney transplant clinic, accounting for 15-20% of these patients. Approximately 10% of such cases may have an underlying monogenic cause of kidney failure. Modern genetic approaches can provide a precise diagnosis for patients and their families. A search for extra-renal disease manifestations is also important as this may point to a specific genetic diagnosis. Here, we present two patients where molecular genetic testing was performed because of kidney failure of unknown aetiology and associated retinal phenotypes. The first patient reached kidney failure at 16 years of age but only presented with a retinal phenotype at 59 years of age and was found to have evidence of rod-cone dystrophy. The second patient presented with childhood kidney failure at the age of 15 years and developed visual difficulties and photophobia at the age of 32 years and was diagnosed with cone dystrophy. In both cases, genetic tests were performed which revealed a homozygous whole-gene deletion of -encoding nephrocystin-1, providing the unifying diagnosis of Senior-Løken syndrome type 1. We conclude that reviewing kidney and extra-renal phenotypes together with targeted genetic testing was informative in these cases of kidney failure of unknown aetiology and associated retinal phenotypes. The involvement of an interdisciplinary team is advisable when managing such patients and allows referral to other relevant specialities. The long time lag and lack of diagnostic clarity and clinical evaluation in our cases should encourage genetic investigations for every young patient with unexplained kidney failure. For these and similar patients, a more timely genetic diagnosis would allow for improved management, a risk assessment of kidney disease in relatives, and the earlier identification of extra-renal disease manifestations.
The online version contains supplementary material available at 10.1007/s44162-024-00031-4.
医学上的精确诊断有助于进行针对特定疾病的恰当管理。病因不明的肾衰竭在血液透析单元和肾移植诊所中仍是常见的诊断标签,占这些患者的15% - 20%。此类病例中约10%可能存在潜在的单基因性肾衰竭病因。现代基因检测方法可为患者及其家属提供精确诊断。寻找肾外疾病表现也很重要,因为这可能指向特定的基因诊断。在此,我们介绍两名因病因不明的肾衰竭及相关视网膜表型而进行分子基因检测的患者。第一名患者16岁时出现肾衰竭,但直到59岁才出现视网膜表型,被发现有视杆 - 视锥营养不良的迹象。第二名患者15岁时出现儿童期肾衰竭,32岁时出现视力困难和畏光症状,被诊断为视锥营养不良。在这两个病例中,基因检测均显示编码nephrocystin - 1的基因存在纯合全基因缺失,从而得出1型Senior - Løken综合征的统一诊断。我们得出结论,在这些病因不明的肾衰竭及相关视网膜表型病例中,综合审视肾脏和肾外表型并进行靶向基因检测是有价值的。在管理此类患者时,建议由多学科团队参与,并允许转诊至其他相关专科。我们病例中的长时间延迟、缺乏诊断清晰度和临床评估情况应促使对每一位病因不明的年轻肾衰竭患者进行基因调查。对于这些及类似患者,更及时的基因诊断将有助于改善管理、对亲属的肾脏疾病进行风险评估以及更早发现肾外疾病表现。
在线版本包含可在10.1007/s44162 - 024 - 00031 - 4获取的补充材料。