Delvau N, Elens L, Penaloza A, Liistro G, Thys F, Roy P M, Gianello P, Hantson P
Department of Emergency Care, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Brussels 1200, Belgium.
Integrated Pharmacometrics, Pharmacogenomics and PharmacoKinetics (PMGK) Research group, Louvain Drug Research Institute (LDRI), Université Catholique de Louvain, Brussels 1200, Belgium.
Toxicol Rep. 2024 Feb 23;12:271-279. doi: 10.1016/j.toxrep.2024.02.005. eCollection 2024 Jun.
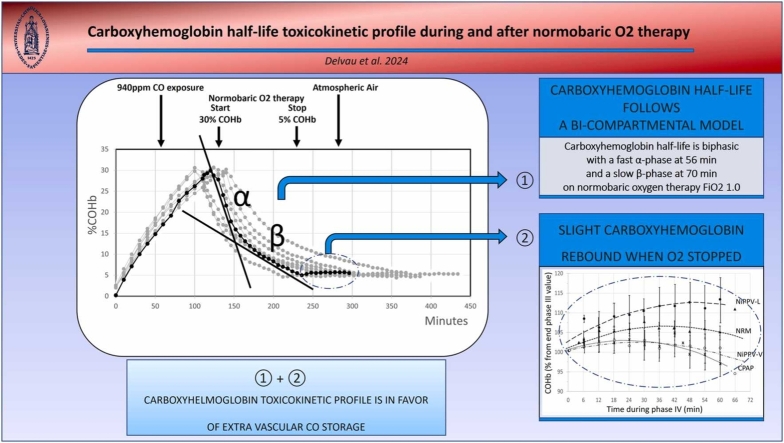
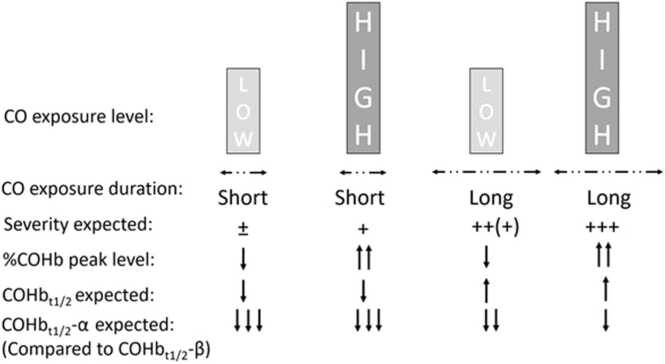
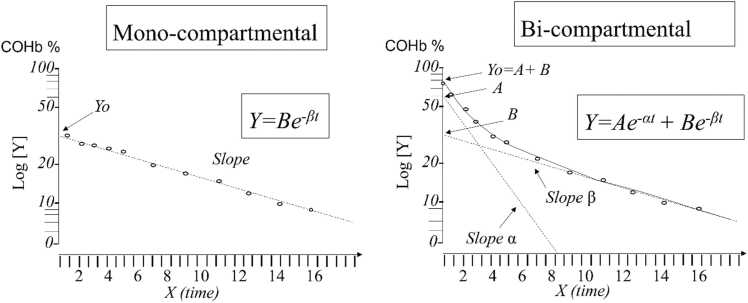
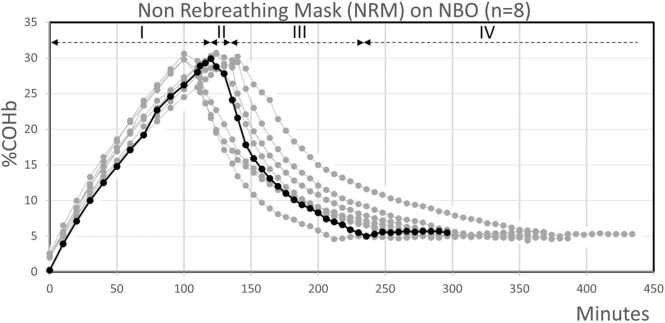
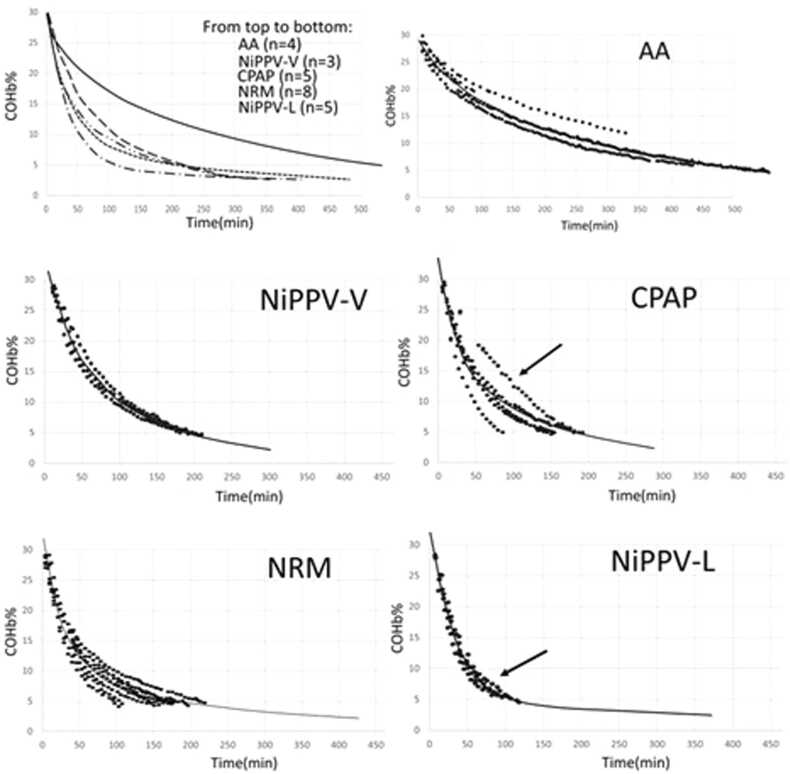
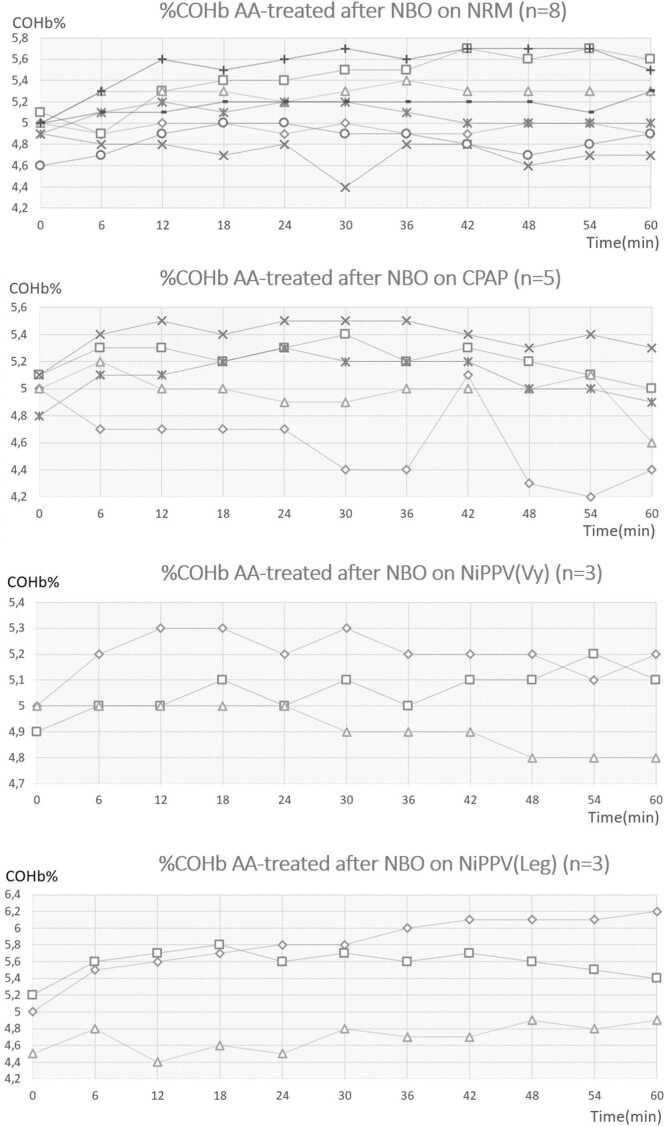
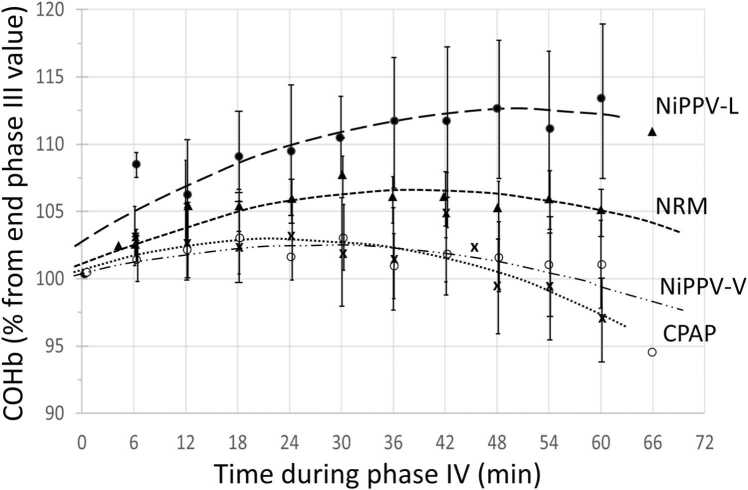
Investigations on acute carbon monoxide (CO) poisoning struggle to highlight a relevant discriminant criterion related to CO poisoning severity for predicting complications, such as delayed neurological syndromes. In this context, it remains difficult to demonstrate the superiority of one method of oxygen (O) administration over others or to identify the optimal duration of normobaric 100% oxygen (NBO) treatment. Myoglobin, as hemoglobin, are a potential binding site for CO, which could be a source of extravascular CO storage that impacts the severity of CO poisoning. It is not possible in routine clinical practice to estimate this potential extravascular CO storage. Indirect means of doing so that are available in the first few hours of poisoning could include, for example, the carboxyhemoglobin half-life (COHb), which seems to be influenced itself by the level and duration of CO exposure affecting this store of CO within the body. However, before the elimination of CO can be assessed, the COHb toxicokinetic model must be confirmed: research still debates whether this model mono- or bi-compartmental. The second indirect mean could be the assessment of a potential COHb rebound after COHb has returned to 5% and NBO treatment has stopped. Moreover, a COHb rebound could be considered to justify the duration of NBO treatment. On an experimental swine model exposed to moderate CO poisoning (940 ppm for ±118 min until COHb reached 30%), we first confirm that the COHb half-life follows a bi-compartmental model. Secondly, we observe for the first time a slight COHb rebound when COHb returns to 5% and oxygen therapy is stopped. On the basis of these two toxicokinetic characteristics in favor of extravascular CO storage, we recommend that COHb is considered using the bi-compartmental model in future clinical studies that compare treatment effectiveness as a potential severity criterion to homogenize cohorts of the same severity. Moreover, from a general toxicokinetic point of view, we confirm that a treatment lasting less than 6 hours appears to be insufficient for treating moderate CO poisoning.
关于急性一氧化碳(CO)中毒的研究难以突出与CO中毒严重程度相关的、用于预测并发症(如迟发性神经综合征)的相关判别标准。在此背景下,仍难以证明一种氧(O)给药方法优于其他方法,或确定常压100%氧(NBO)治疗的最佳持续时间。肌红蛋白与血红蛋白一样,是CO的潜在结合位点,这可能是血管外CO储存的一个来源,会影响CO中毒的严重程度。在常规临床实践中,无法估计这种潜在的血管外CO储存量。在中毒后的最初几个小时内可用的间接估计方法可能包括,例如,碳氧血红蛋白半衰期(COHb),它似乎本身也受到影响体内CO储存的CO暴露水平和持续时间的影响。然而,在评估CO的消除之前,必须确认COHb毒代动力学模型:研究仍在争论该模型是单室还是双室的。第二种间接方法可能是在COHb恢复到5%且NBO治疗停止后,评估潜在的COHb反弹。此外,COHb反弹可被视为证明NBO治疗持续时间合理的依据。在暴露于中度CO中毒(940 ppm,持续约118分钟直至COHb达到30%)的实验猪模型中,我们首先证实COHb半衰期遵循双室模型。其次,我们首次观察到当COHb恢复到5%且氧疗停止时,会出现轻微的COHb反弹。基于这两个有利于血管外CO储存的毒代动力学特征,我们建议在未来比较治疗效果的临床研究中,将COHb视为使用双室模型,作为潜在的严重程度标准,以使相同严重程度的队列同质化。此外,从一般毒代动力学角度来看,我们证实持续时间少于6小时的治疗似乎不足以治疗中度CO中毒。