Department of Trauma Surgery, War Trauma Medical Center, State Key Laboratory of Trauma, Burn and Combined Injury, Daping Hospital, Army Medical University, Chongqing, 400042, China.
Eur J Med Res. 2024 Mar 6;29(1):153. doi: 10.1186/s40001-024-01760-4.
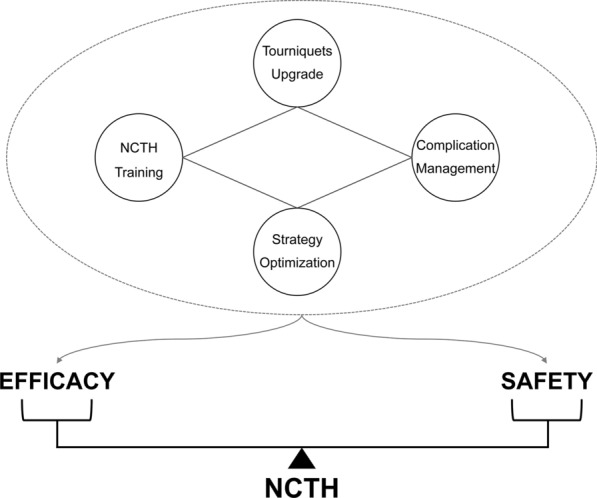
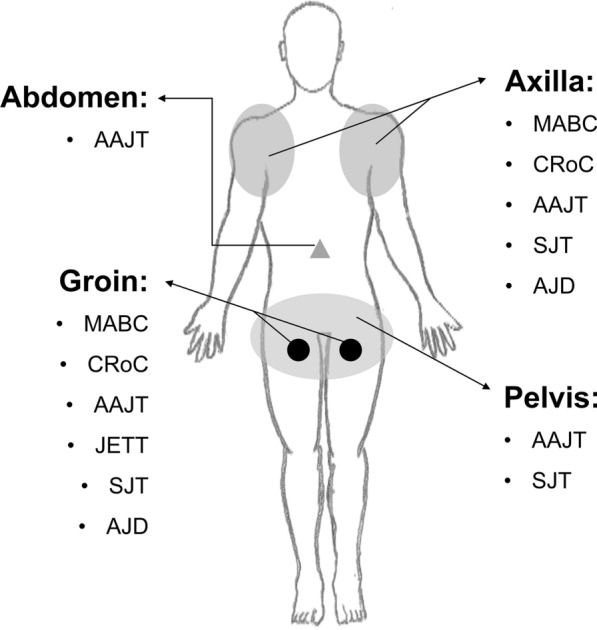
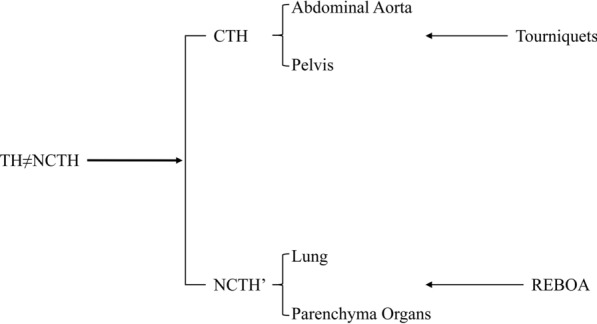
Since limb bleeding has been well managed by extremity tourniquets, the management of exsanguinating torso hemorrhage (TH) has become a hot issue both in military and civilian medicine. Conventional hemostatic techniques are ineffective for managing traumatic bleeding of organs and vessels within the torso due to the anatomical features. The designation of noncompressible torso hemorrhage (NCTH) marks a significant step in investigating the injury mechanisms and developing effective methods for bleeding control. Special tourniquets such as abdominal aortic and junctional tourniquet and SAM junctional tourniquet designed for NCTH have been approved by FDA for clinical use. Combat ready clamp and junctional emergency treatment tool also exhibit potential for external NCTH control. In addition, resuscitative endovascular balloon occlusion of the aorta (REBOA) further provides an endovascular solution to alleviate the challenges of NCTH treatment. Notably, NCTH cognitive surveys have revealed that medical staff have deficiencies in understanding relevant concepts and treatment abilities. The stereotypical interpretation of NCTH naming, particularly the term noncompressible, is the root cause of this issue. This review discusses the dynamic relationship between TH and NCTH by tracing the development of external NCTH control techniques. The authors propose to further subdivide the existing NCTH into compressible torso hemorrhage and NCTH' (noncompressible but REBOA controllable) based on whether hemostasis is available via external compression. Finally, due to the irreplaceability of special tourniquets during the prehospital stage, the authors emphasize the importance of a package program to improve the efficacy and safety of external NCTH control. This program includes the promotion of tourniquet redesign and hemostatic strategies, personnel reeducation, and complications prevention.
由于肢体出血已通过四肢止血带得到很好的控制,因此在外伤性胸部出血(TH)的管理方面,无论是在军事医学还是民用医学领域都成为了一个热点问题。由于解剖学特征,常规止血技术对于控制胸内器官和血管的创伤性出血无效。非可压缩性胸出血(NCTH)的指定标志着在研究损伤机制和开发有效止血方法方面迈出了重要一步。专门为 NCTH 设计的腹主动脉和结部止血带和 SAM 结部止血带等特殊止血带已获得 FDA 批准用于临床使用。用于外部 NCTH 控制的 ready clamp 和 junctional emergency treatment tool 也具有潜在的应用前景。此外,复苏性血管内主动脉球囊阻断(REBOA)进一步为缓解 NCTH 治疗挑战提供了血管内解决方案。值得注意的是,NCTH 认知调查显示,医务人员在理解相关概念和治疗能力方面存在不足。对 NCTH 命名的刻板解释,尤其是“非可压缩性”一词,是造成这一问题的根本原因。本综述通过追踪外部 NCTH 控制技术的发展,讨论了 TH 和 NCTH 之间的动态关系。作者建议根据是否通过外部压迫实现止血,将现有的 NCTH 进一步细分为可压缩性胸出血和 NCTH'(不可压缩但可通过 REBOA 控制)。最后,由于在院前阶段特殊止血带的不可替代性,作者强调了改进外部 NCTH 控制的功效和安全性的一揽子计划的重要性。该方案包括促进止血带重新设计和止血策略、人员再教育以及预防并发症。