NIHR Policy Research Unit in Behavioural Science, Newcastle University, Newcastle upon Tyne, UK.
School of Psychology, University of Leeds, Leeds, UK.
BMJ Open. 2024 Mar 7;14(3):e067252. doi: 10.1136/bmjopen-2022-067252.
To examine the effectiveness of shared medical appointments (SMAs) compared with one-to-one appointments in primary care for improving health outcomes and reducing demand on healthcare services by people with one or more long-term conditions (LTCs).
A systematic review of the published literature.
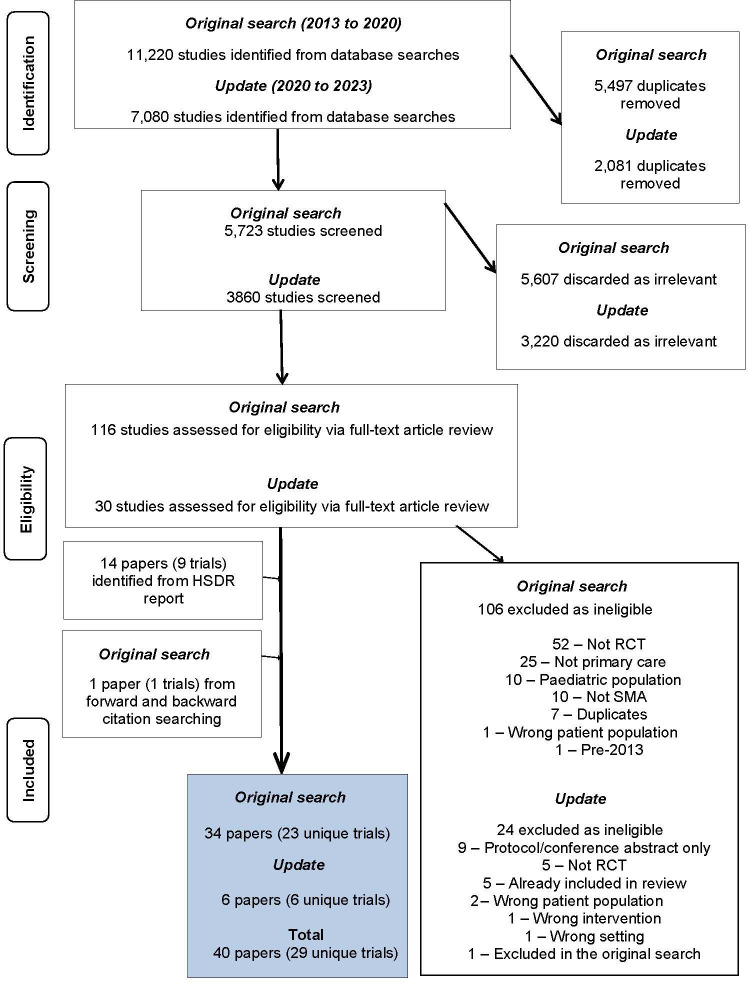
Six databases, including MEDLINE and Web of Science, were searched 2013-2023. Relevant pre-2013 trials identified by forward and backward citation searches of the included trials were included.
Randomised controlled trials of SMAs delivered in a primary care setting involving adults over 18 years with one or more LTCs. Studies were excluded if the SMA did not include one-to-one patient-clinician time. All countries were eligible for inclusion.
Data were extracted and outcomes narratively synthesised, meta-analysis was undertaken where possible.
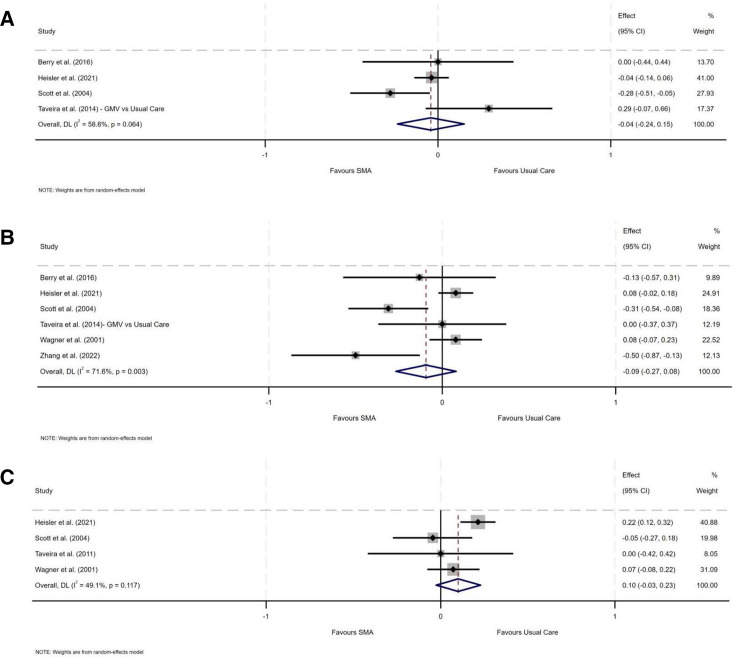
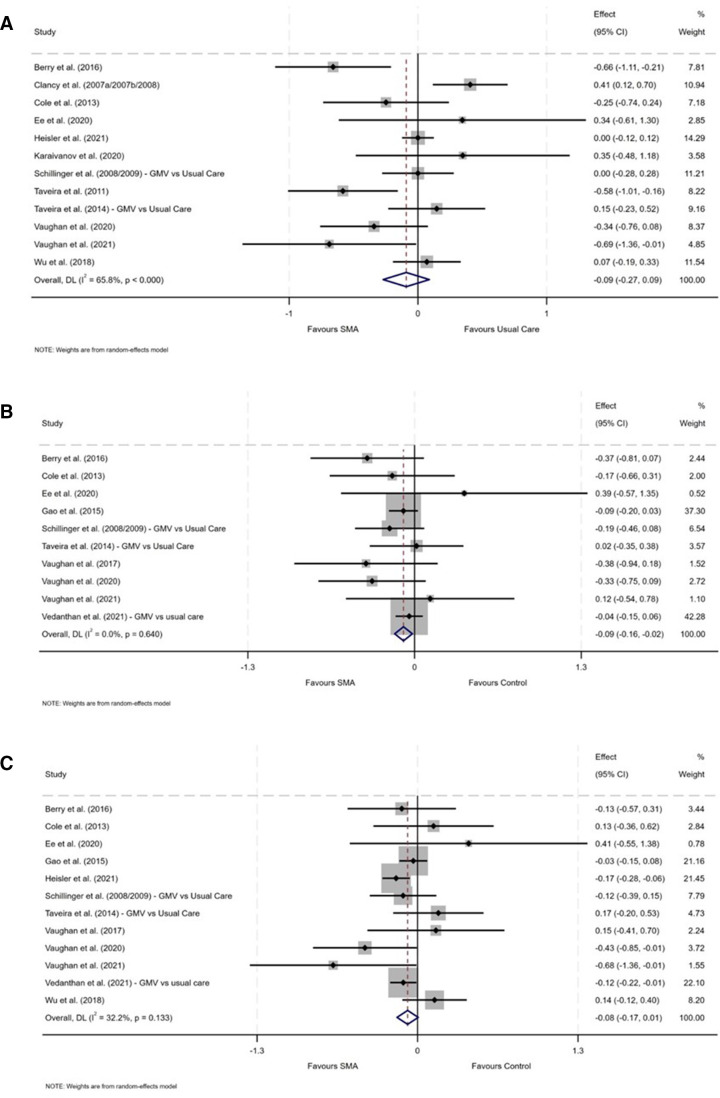
Twenty-nine unique trials were included. SMA models varied in terms of components, mode of delivery and target population. Most trials recruited patients with a single LTC, most commonly diabetes (n=16). There was substantial heterogeneity in outcome measures. Meta-analysis showed that participants in SMA groups had lower diastolic blood pressure than those in usual care (d=-0.086, 95% CI=-0.16 to -0.02, n=10) (p=0.014). No statistically significant differences were found across other outcomes. Compared with usual care, SMAs had no significant effect on healthcare service use. For example, no difference between SMAs and usual care was found for admissions to emergency departments at follow-up (d=-0.094, 95% CI=-0.27 to 0.08, n=6, p=0.289).
There was a little difference in the effectiveness of SMAs compared with usual care in terms of health outcomes or healthcare service use in the short-term (range 12 weeks to 24 months). To strengthen the evidence base, future studies should include a wider array of LTCs, standardised outcome measures and more details on SMA components to help inform economic evaluation.
CRD42020173084.
探讨在初级保健中,与一对一预约相比,共病患者的共享医疗预约(SMA)对改善健康结果和减少医疗服务需求的有效性。
对已发表文献的系统评价。
2013 年至 2023 年,共检索了 6 个数据库,包括 MEDLINE 和 Web of Science。纳入试验的前瞻性和回溯性引文搜索中确定了相关的预 2013 年试验。
在初级保健环境中进行的 SMA 随机对照试验,涉及 18 岁以上患有一种或多种慢性病(LTCs)的成年人。如果 SMA 不包括一对一的医患时间,则排除该试验。所有国家均符合纳入标准。
提取数据并进行结果叙述性综合,在可能的情况下进行荟萃分析。
共纳入 29 项独特的试验。SMA 模型在组成部分、传递方式和目标人群方面存在差异。大多数试验招募了患有单一 LTC 的患者,最常见的是糖尿病(n=16)。结局测量指标存在很大的异质性。荟萃分析显示,SMA 组患者的舒张压低于常规护理组(d=-0.086,95%CI=-0.16 至-0.02,n=10)(p=0.014)。其他结局没有发现统计学意义上的差异。与常规护理相比,SMA 对医疗服务的使用没有显著影响。例如,在随访时,SMA 与常规护理之间在急诊科入院方面没有差异(d=-0.094,95%CI=-0.27 至 0.08,n=6,p=0.289)。
在短期(12 周至 24 个月)内,与常规护理相比,SMA 在健康结果或医疗服务使用方面的效果差异不大。为了加强证据基础,未来的研究应包括更广泛的 LTCs、标准化的结局测量指标以及更详细的 SMA 组成部分,以帮助进行经济评估。
PROSPERO 注册号:CRD42020173084。