Chen Zhi-Ren, Yang Mei-Fang, Xie Zhi-Yuan, Wang Pei-An, Zhang Liang, Huang Ze-Hua, Luo Yao
Department of Science and Education, Xuzhou Medical University, Xuzhou Clinical College, Xuzhou 221000, Jiangsu Province, China.
Department of Neurology, Xuzhou Medical University, Xuzhou 221000, Jiangsu Province, China.
World J Gastrointest Surg. 2024 Feb 27;16(2):357-381. doi: 10.4240/wjgs.v16.i2.357.
Gastric cancer (GC) is prevalent and aggressive, especially when patients have distant lung metastases, which often places patients into advanced stages. By identifying prognostic variables for lung metastasis in GC patients, it may be possible to construct a good prediction model for both overall survival (OS) and the cumulative incidence prediction (CIP) plot of the tumour.
To investigate the predictors of GC with lung metastasis (GCLM) to produce nomograms for OS and generate CIP by using cancer-specific survival (CSS) data.
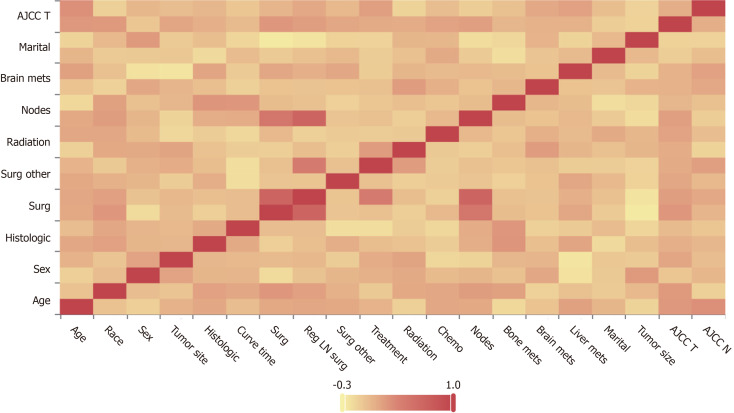
Data from January 2000 to December 2020 involving 1652 patients with GCLM were obtained from the Surveillance, epidemiology, and end results program database. The major observational endpoint was OS; hence, patients were separated into training and validation groups. Correlation analysis determined various connections. Univariate and multivariate Cox analyses validated the independent predictive factors. Nomogram distinction and calibration were performed with the time-dependent area under the curve (AUC) and calibration curves. To evaluate the accuracy and clinical usefulness of the nomograms, decision curve analysis (DCA) was performed. The clinical utility of the novel prognostic model was compared to that of the 7 edition of the American Joint Committee on Cancer (AJCC) staging system by utilizing Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI). Finally, the OS prognostic model and Cox-AJCC risk stratification model modified for the AJCC system were compared.
For the purpose of creating the OS nomogram, a CIP plot based on CSS was generated. Cox multivariate regression analysis identified eleven significant prognostic factors ( < 0.05) related to liver metastasis, bone metastasis, primary site, surgery, regional surgery, treatment sequence, chemotherapy, radiotherapy, positive lymph node count, N staging, and time from diagnosis to treatment. It was clear from the DCA (net benefit > 0), time-dependent ROC curve (training/validation set AUC > 0.7), and calibration curve (reliability slope closer to 45 degrees) results that the OS nomogram demonstrated a high level of predictive efficiency. The OS prediction model (New Model AUC = 0.83) also performed much better than the old Cox-AJCC model (AUC difference between the new model and the old model greater than 0) in terms of risk stratification ( < 0.0001) and verification using the IDI and NRI.
The OS nomogram for GCLM successfully predicts 1- and 3-year OS. Moreover, this approach can help to appropriately classify patients into high-risk and low-risk groups, thereby guiding treatment.
胃癌(GC)普遍存在且具有侵袭性,尤其是当患者出现远处肺转移时,这通常会使患者进入晚期阶段。通过识别GC患者肺转移的预后变量,有可能构建一个良好的总生存期(OS)预测模型和肿瘤累积发病率预测(CIP)图。
研究GC伴肺转移(GCLM)的预测因素,以制作OS列线图,并使用癌症特异性生存(CSS)数据生成CIP。
从监测、流行病学和最终结果计划数据库中获取2000年1月至2020年12月期间涉及1652例GCLM患者的数据。主要观察终点为OS;因此,将患者分为训练组和验证组。相关性分析确定了各种关联。单因素和多因素Cox分析验证了独立预测因素。使用曲线下时间依赖性面积(AUC)和校准曲线进行列线图区分和校准。为了评估列线图的准确性和临床实用性,进行了决策曲线分析(DCA)。通过利用净重新分类改善(NRI)和综合判别改善(IDI),将新的预后模型的临床实用性与美国癌症联合委员会(AJCC)第7版分期系统的临床实用性进行了比较。最后,比较了OS预后模型和针对AJCC系统修改的Cox-AJCC风险分层模型。
为了创建OS列线图,生成了基于CSS的CIP图。Cox多因素回归分析确定了11个与肝转移、骨转移、原发部位、手术、区域手术、治疗顺序、化疗、放疗、阳性淋巴结计数、N分期以及从诊断到治疗的时间相关的显著预后因素(<0.05)。从DCA(净效益>0)、时间依赖性ROC曲线(训练/验证集AUC>0.7)和校准曲线(可靠性斜率更接近45度)结果可以明显看出,OS列线图显示出高水平的预测效率。在风险分层(<0.0001)以及使用IDI和NRI进行验证方面,OS预测模型(新模型AUC = 0.83)也比旧的Cox-AJCC模型(新模型与旧模型之间的AUC差异大于0)表现得好得多。
GCLM的OS列线图成功预测了1年和3年的OS。此外,这种方法有助于将患者适当地分为高风险和低风险组,从而指导治疗。