Alotaibi Mona, Yang Jenny Z, Papamatheakis Demosthenes G, McGuire W Cameron, Fernandes Timothy M, Morris Timothy A
Division of Pulmonary, Critical Care and Sleep Medicine, University of California, San Diego Healthcare, 200 West Arbor Drive, San Diego, CA, 92103-8378, USA.
Respir Res. 2024 Mar 11;25(1):121. doi: 10.1186/s12931-024-02746-w.
Cardiac dysfunction from pulmonary vascular disease causes characteristic findings on cardiopulmonary exercise testing (CPET). We tested the accuracy of CPET for detecting inadequate stroke volume (SV) augmentation during exercise, a pivotal manifestation of cardiac limitation in patients with pulmonary vascular disease.
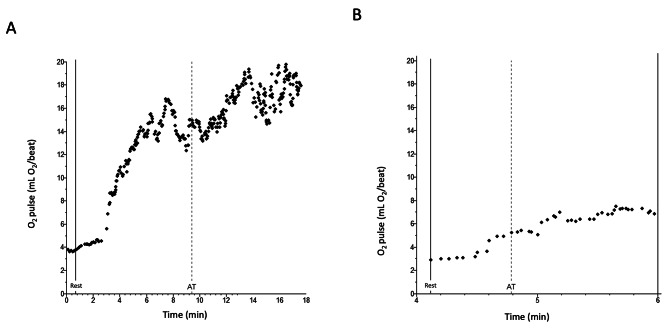
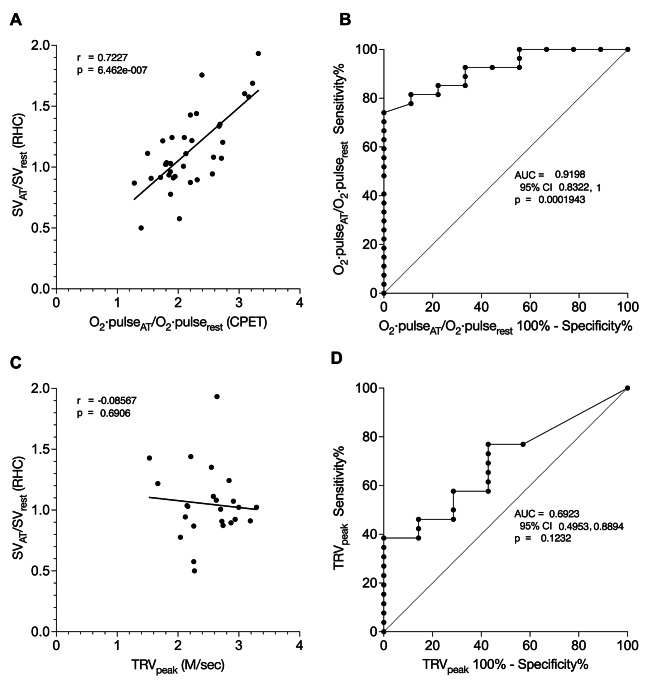
We reviewed patients with suspected pulmonary vascular disease in whom CPET and right heart catheterization (RHC) measurements were taken at rest and at anaerobic threshold (AT). We correlated CPET-determined O·pulse/O·pulse with RHC-determined SV/SV. We evaluated the sensitivity and specificity of O·pulse/O·pulse to detect SV/SV below the lower limit of normal (LLN). For comparison, we performed similar analyses comparing echocardiographically-measured peak tricuspid regurgitant velocity (TRV) with SV/SV.
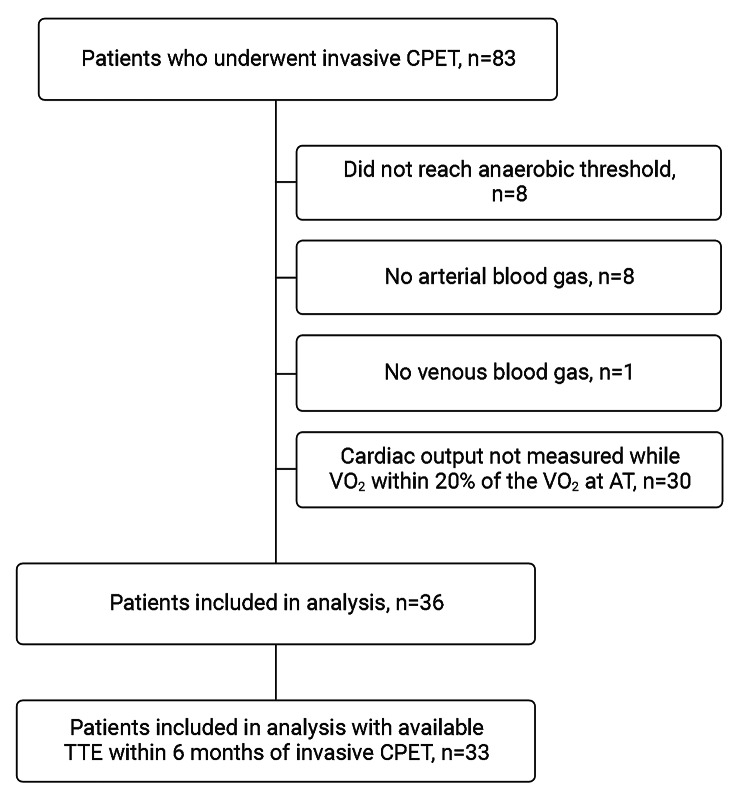
From July 2018 through February 2023, 83 simultaneous RHC and CPET were performed. Thirty-six studies measured O·pulse and SV at rest and at AT. O·pulse/O·pulse correlated highly with SV/SV (r = 0.72, 95% CI 0.52, 0.85; p < 0.0001), whereas TRV did not (r = -0.09, 95% CI -0.47, 0.33; p = 0.69). The AUROC to detect SV/SV below the LLN was significantly higher for O·pulse/O·pulse (0.92, SE 0.04; p = 0.0002) than for TRV (0.69, SE 0.10; p = 0.12). O·pulse/O·pulse of less than 2.6 was 92.6% sensitive (95% CI 76.6%, 98.7%) and 66.7% specific (95% CI 35.2%, 87.9%) for deficient SV/SV.
CPET detected deficient SV augmentation more accurately than echocardiography. CPET-determined O·pulse/O·pulse may have a prominent role for noninvasive screening of patients at risk for pulmonary vascular disease, such as patients with persistent dyspnea after pulmonary embolism.
肺血管疾病导致的心脏功能障碍在心肺运动试验(CPET)中会产生特征性表现。我们测试了CPET检测运动期间每搏输出量(SV)增加不足的准确性,这是肺血管疾病患者心脏受限的一个关键表现。
我们回顾了疑似肺血管疾病的患者,这些患者在静息状态和无氧阈值(AT)时进行了CPET和右心导管检查(RHC)测量。我们将CPET测定的O·脉搏/O·脉搏与RHC测定的SV/SV进行关联。我们评估了O·脉搏/O·脉搏检测低于正常下限(LLN)的SV/SV的敏感性和特异性。为了进行比较,我们进行了类似的分析,将超声心动图测量的三尖瓣反流峰值速度(TRV)与SV/SV进行比较。
从2018年7月到2023年2月,共进行了83次同步的RHC和CPET。36项研究在静息状态和AT时测量了O·脉搏和SV。O·脉搏/O·脉搏与SV/SV高度相关(r = 0.72,95%可信区间0.52,0.85;p < 0.0001),而TRV则不然(r = -0.09,95%可信区间-0.47,0.33;p = 0.69)。检测低于LLN的SV/SV时,O·脉搏/O·脉搏的曲线下面积(AUROC)显著高于TRV(0.92,标准误0.04;p = 0.0002)(0.69,标准误0.10;p = 0.12)。O·脉搏/O·脉搏小于2.6时,对SV/SV不足的敏感性为92.6%(95%可信区间76.6%,98.7%),特异性为66.7%(95%可信区间35.2%,87.9%)。
CPET比超声心动图更准确地检测到SV增加不足。CPET测定的O·脉搏/O·脉搏可能在对肺血管疾病风险患者(如肺栓塞后持续呼吸困难的患者)进行无创筛查中发挥重要作用。