Department of Emergency Medicine, Al-Thawra Modern General Teaching Hospital, Sana'a City, Yemen.
Faculty of Medicine, Al-Azhar University, Cairo, Egypt.
Syst Rev. 2024 Mar 12;13(1):85. doi: 10.1186/s13643-024-02500-9.
Intubating a patient in an emergent setting presents significant challenges compared to planned intubation in an operating room. This study aims to compare video laryngoscopy versus direct laryngoscopy in achieving successful endotracheal intubation on the first attempt in emergency intubations, irrespective of the clinical setting.
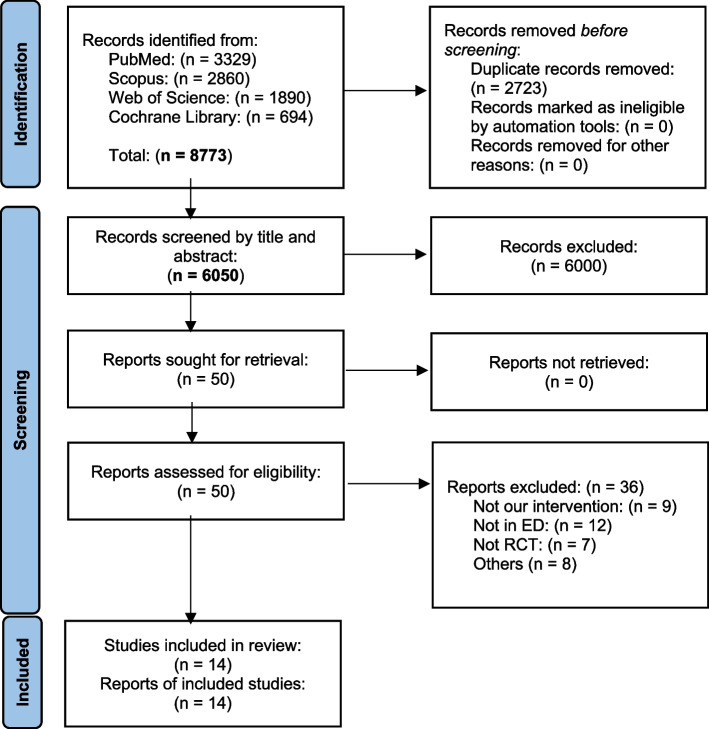
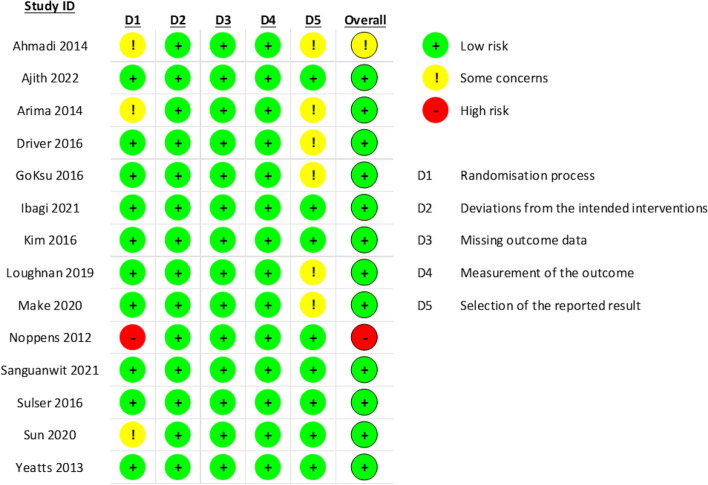
We systematically searched PubMed, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials from inception until 27 February 2023. We included only randomized controlled trials that included patients who had undergone emergent endotracheal intubation for any indication, regardless of the clinical setting. We used the Cochrane risk-of-bias assessment tool 2 (ROB2) to assess the included studies. We used the mean difference (MD) and risk ratio (RR), with the corresponding 95% confidence interval (CI), to pool the continuous and dichotomous variables, respectively.
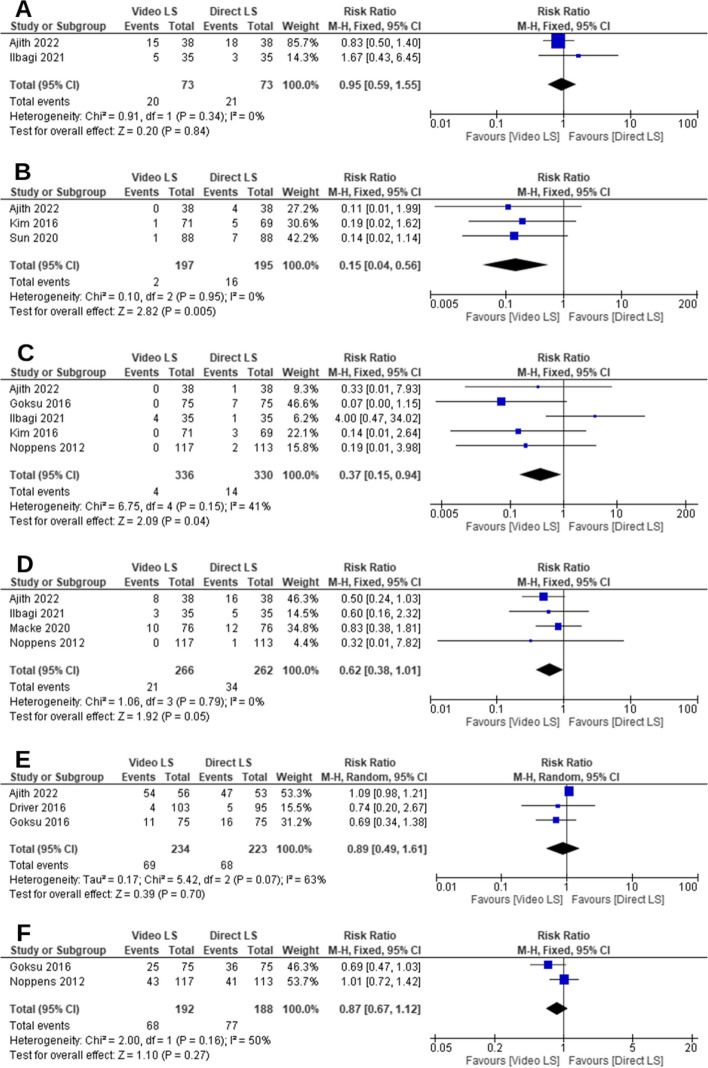
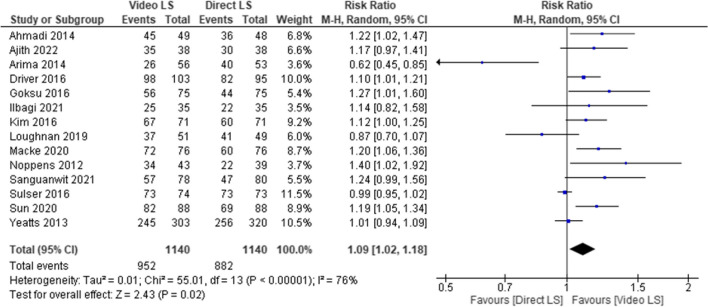
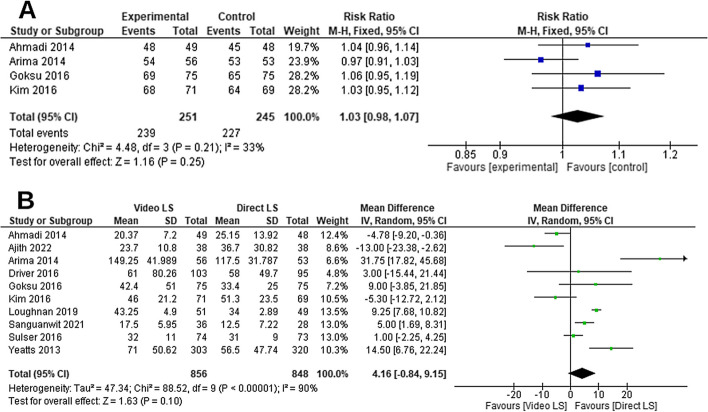
Fourteen studies were included with a total of 2470 patients. The overall analysis favored video laryngoscopy over direct laryngoscopy in first-attempt success rate (RR = 1.09, 95% CI [1.02, 1.18], P = 0.02), first-attempt intubation time (MD = - 6.92, 95% CI [- 12.86, - 0.99], P = 0.02), intubation difficulty score (MD = - 0.62, 95% CI [- 0.86, - 0.37], P < 0.001), peri-intubation percentage of glottis opening (MD = 24.91, 95% CI [11.18, 38.64], P < 0.001), upper airway injuries (RR = 0.15, 95% CI [0.04, 0.56], P = 0.005), and esophageal intubation (RR = 0.37, 95% CI [0.15, 0.94], P = 0.04). However, no difference between the two groups was found regarding the overall intubation success rate (P > 0.05).
In emergency intubations, video laryngoscopy is preferred to direct laryngoscopy in achieving successful intubation on the first attempt and was associated with a lower incidence of complications.
与手术室中的计划性插管相比,在紧急情况下为患者插管具有更大的挑战性。本研究旨在比较视频喉镜与直接喉镜在实现紧急插管时首次尝试气管内插管成功的效果,无论临床环境如何。
我们系统地检索了 PubMed、Scopus、Web of Science 和 Cochrane 对照试验中心注册库,检索时间从建库至 2023 年 2 月 27 日。我们仅纳入了那些为任何适应证而接受紧急气管插管的患者的随机对照试验,无论临床环境如何。我们使用 Cochrane 偏倚风险评估工具 2(ROB2)来评估纳入的研究。我们使用均数差(MD)和风险比(RR)及其相应的 95%置信区间(CI)分别汇总连续和二分类变量。
共纳入 14 项研究,总计 2470 例患者。总体分析结果表明,与直接喉镜相比,视频喉镜在首次尝试成功率(RR=1.09,95%CI [1.02,1.18],P=0.02)、首次插管时间(MD=-6.92,95%CI [-12.86,-0.99],P=0.02)、插管难度评分(MD=-0.62,95%CI [-0.86,-0.37],P<0.001)、声门开放程度(MD=24.91,95%CI [11.18,38.64],P<0.001)、上呼吸道损伤(RR=0.15,95%CI [0.04,0.56],P=0.005)和食管插管(RR=0.37,95%CI [0.15,0.94],P=0.04)方面更具优势。然而,两组的总体插管成功率无差异(P>0.05)。
在紧急插管中,与直接喉镜相比,视频喉镜在首次尝试时更有助于实现成功插管,且并发症发生率更低。