Division of Renal Medicine, CLINTEC, Karolinska Institutet, Stockholm, Sweden.
Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands.
Nephrol Dial Transplant. 2024 Nov 27;39(12):2079-2087. doi: 10.1093/ndt/gfae064.
Risk-based thresholds for arteriovenous (AV) access creation has been proposed to aid vascular access planning. We aimed to assess the clinical impact of implementing the Kidney Failure Risk Equation (KFRE) for vascular access referral.
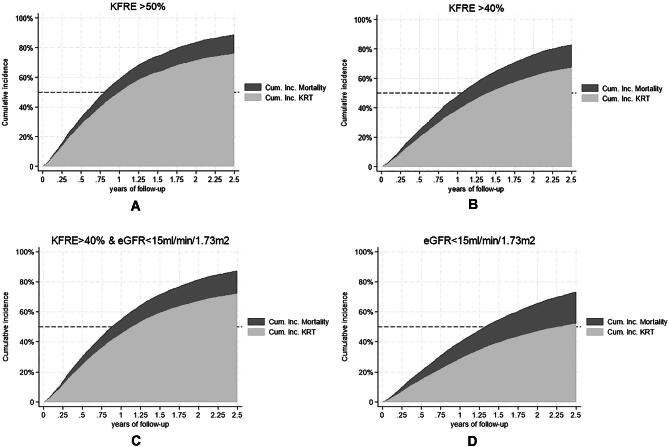
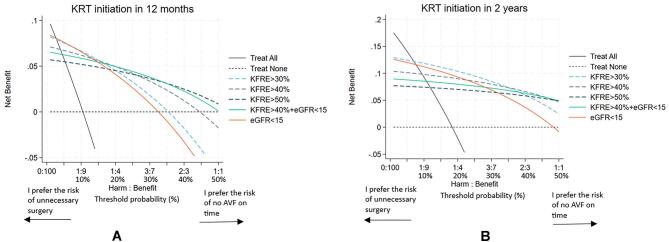
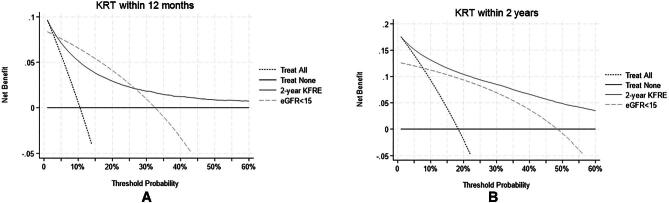
A total of 16 102 nephrology-referred chronic kidney disease (CKD) patients from the Swedish Renal Registry 2008-18 were included. The KFRE was calculated repeatedly, and the timing was identified for when the KFRE risk exceeded several pre-defined thresholds and/or the estimated glomerular filtration rate was <15 mL/min/1.73 m2 (eGFR15). To assess the utility of the KFRE/eGFR thresholds, cumulative incidence curves of kidney replacement therapy (KRT) or death, and decision-curve analyses were computed at 6 and 12 months, and 2 years. The potential impact of using the different thresholds was illustrated by an example from the Swedish access registry.
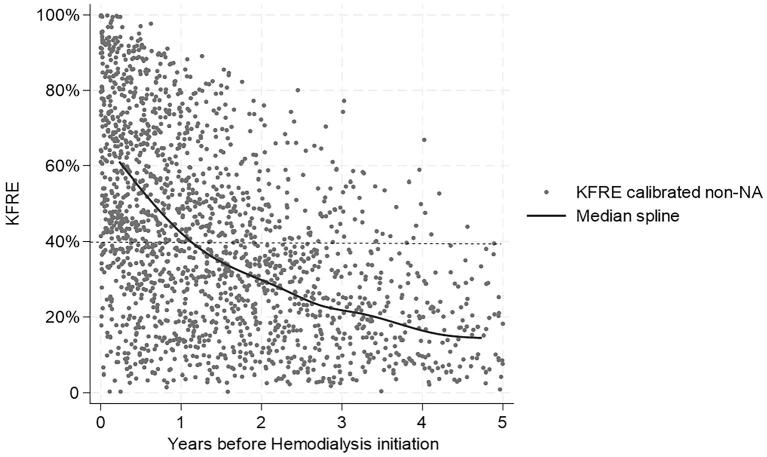
The 12-month specificity for KRT initiation was highest for KFRE >50% {94.5 [95% confidence interval (CI) 94.3-94.7]} followed by KFRE >40% [90.0 (95% CI 89.7-90.3)], while sensitivity was highest for KFRE >30% [79.3 (95% CI 78.2-80.3)] and eGFR <15 mL/min/1.73 m2 [81.2 (95% CI 80.2-82.2)]. The 2-year positive predictive value was 71.5 (95% CI 70.2-72.8), 61.7 (95% CI 60.4-63.0) and 47.2 (95% CI 46.1-48.3) for KFRE >50%, KFRE >40% and eGFR <15, respectively. Decision curve analyses suggested the largest net benefit for KFRE >40% over 2 years and KFRE >50% over 12 months when it is important to avoid the harm of possibly unnecessary surgery. In Sweden, 54% of nephrology-referred patients started hemodialysis in a central venous catheter (CVC), of whom only 5% had AV access surgery >6 months before initiation. Sixty percent of the CVC patients exceeded KFRE >40% a median of 0.8 years (interquartile range 0.4-1.5) before KRT initiation.
The utility of using KFRE >40% and KFRE >50% is higher compared with the more traditionally used eGFR threshold <15 mL/min/1.73 m2 for vascular access planning.
为了辅助血管通路规划,已经提出了基于风险的动静脉(AV)通路创建阈值。我们旨在评估实施肾脏病预后方程(KFRE)进行血管通路转介的临床影响。
纳入了来自瑞典肾脏登记处 2008-2018 年的 16102 例接受肾脏病转诊的慢性肾脏病(CKD)患者。反复计算 KFRE,并确定何时 KFRE 风险超过几个预先定义的阈值和/或估计肾小球滤过率(eGFR15)<15 mL/min/1.73 m2。为了评估 KFRE/eGFR 阈值的效用,在 6、12 个月和 2 年时计算了肾脏替代治疗(KRT)或死亡的累积发病率曲线和决策曲线分析。通过瑞典通路登记处的一个示例说明了使用不同阈值的潜在影响。
在 KRT 启动的 12 个月特异性方面,KFRE >50%[94.5(95%置信区间 94.3-94.7)]最高,其次是 KFRE >40%[90.0(95%置信区间 94.7-90.3)],而敏感性最高的是 KFRE >30%[79.3(95%置信区间 78.2-80.3)]和 eGFR <15 mL/min/1.73 m2[81.2(95%置信区间 80.2-82.2)]。在 2 年时,KFRE >50%、KFRE >40%和 eGFR <15 的阳性预测值分别为 71.5(95%置信区间 70.2-72.8)、61.7(95%置信区间 60.4-63.0)和 47.2(95%置信区间 46.1-48.3)。决策曲线分析表明,在 2 年内,KFRE >40%和 KFRE >50%的净获益最大,在 12 个月内,KFRE >50%的净获益最大,因为这对于避免可能不必要的手术带来的危害很重要。在瑞典,54%接受肾脏病转诊的患者开始在中心静脉导管(CVC)中进行血液透析,其中只有 5%的患者在开始前 6 个月以上进行了动静脉通路手术。60%的 CVC 患者在开始 KRT 前的中位时间(四分位间距 0.4-1.5)内超过了 KFRE >40%。
与更传统的使用 eGFR <15 mL/min/1.73 m2 阈值相比,使用 KFRE >40%和 KFRE >50%进行血管通路规划的效用更高。