Department of Surgery, Kaohsiung Chang Gung Memorial Hospital, 123 Ta-Pei Road, Niao-Song, Kaohsiung, 833, Taiwan.
Chang Gung University College of Medicine, Taoyüan, Taiwan.
Updates Surg. 2024 Aug;76(4):1213-1221. doi: 10.1007/s13304-024-01782-x. Epub 2024 Mar 17.
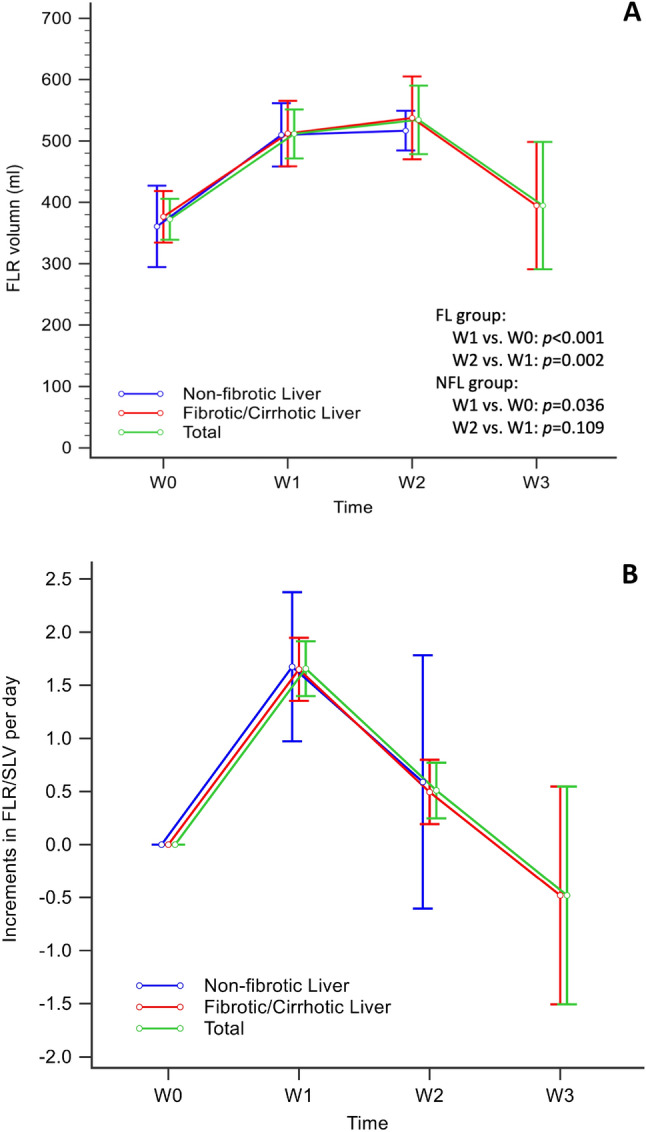
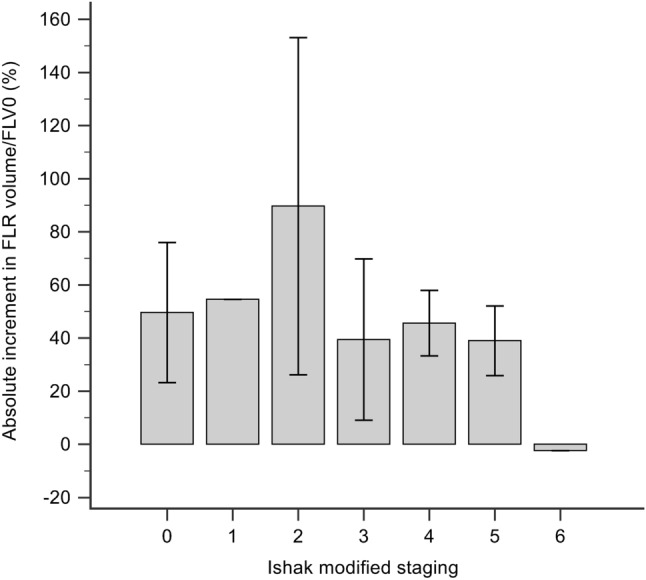
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is a novel procedure for major resection in patients with insufficient future liver remnant (FLR). Effective FLR augmentation is pivotal in the completion of ALPPS. Liver fibrosis/cirrhosis associated with chronic viral hepatitis impairs liver regeneration. To investigate the augmentation of FLR in associating ALPPS between patients with fibrotic/cirrhotic livers (FL) and non-fibrotic livers (NFL) and compare their short-term clinical outcomes and long-term survival. Patients were divided into two groups based on the Ishak modified staging: non-fibrotic liver group (NFL, stage 0) and fibrotic/cirrhotic liver group (FL, stage 1-5/6). Weekly liver regeneration in FLR, perioperative data, and survival outcomes were investigated. Twenty-seven patients with liver tumors underwent ALPPS (NFL, n = 7; FL, n = 20). NFL and FL patients had viral hepatitis (28.6% [n = 2] and 95% [n = 19]), absolute FLR volume increments of 134.90 ml and 161.85 ml (p = 0.825), and rates of hypertrophy were 16.46 ml/day and 13.66 ml/day (p = 0.507), respectively. In the FL group, baseline FLR volume was 360.13 ml, postoperatively it increased to a plateau (542.30 ml) in week 2 and declined (378.45 ml) in week 3. One patient (3.7%) with cirrhotic liver (stage 6) failed to proceed to ALPPS-II. The overall ALPPS-related major complication rate was 7.4%. ALPPS is feasible for fibrotic liver patients classified by Ishak modified stages ≤ 5. After ALPPS-I, 14 days for FLR augmentation seems an appropriate waiting time to reach a maximum FLR volume in these patients.
联合肝脏离断和门静脉结扎的二步肝切除术(ALPPS)是一种针对未来剩余肝脏(FLR)不足的患者进行大切除的新方法。有效的 FLR 增加是完成 ALPPS 的关键。慢性病毒性肝炎相关的肝纤维化/肝硬化会损害肝脏再生。为了研究纤维化/肝硬化(FL)和非纤维化(NFL)患者的 ALPPS 中 FLR 的增加,并比较他们的短期临床结果和长期生存情况,我们将患者根据 Ishak 改良分期分为两组:非纤维化肝脏组(NFL,0 期)和纤维化/肝硬化肝脏组(FL,1-5/6 期)。研究了每周 FLR 的再生情况、围手术期数据和生存结果。27 例肝肿瘤患者接受了 ALPPS(NFL,n=7;FL,n=20)。NFL 和 FL 患者均患有病毒性肝炎(28.6%[n=2]和 95%[n=19]),绝对 FLR 体积增加分别为 134.90ml 和 161.85ml(p=0.825),肝体积增加率分别为 16.46ml/天和 13.66ml/天(p=0.507)。在 FL 组中,基线 FLR 体积为 360.13ml,术后第 2 周增加到平台期(542.30ml),第 3 周下降(378.45ml)。1 例(3.7%)肝硬化(6 期)患者未能进行 ALPPS-II。ALPPS 相关的主要并发症发生率为 7.4%。ALPPS 对于 Ishak 改良分期≤5 的纤维化肝脏患者是可行的。在 ALPPS-I 后,14 天似乎是这些患者达到最大 FLR 体积的适当等待时间。