Nekanti Usha, Sakthivel Pooja S, Zahedi Atena, Creasman Dana A, Nishi Rebecca A, Dumont Courtney M, Piltti Katja M, Guardamondo Glenn L, Hernandez Norbert, Chen Xingyuan, Song Hui, Lin Xiaoxiao, Martinez Joshua, On Lillian, Lakatos Anita, Pawar Kiran, David Brian T, Guo Zhiling, Seidlits Stephanie K, Xu Xiangmin, Shea Lonnie D, Cummings Brian J, Anderson Aileen J
Sue and Bill Gross Stem Cell Research Center, University of California, Irvine, CA, USA.
Department of Anatomy and Neurobiology, University of California, Irvine, CA, USA.
NPJ Regen Med. 2024 Mar 18;9(1):12. doi: 10.1038/s41536-024-00356-0.
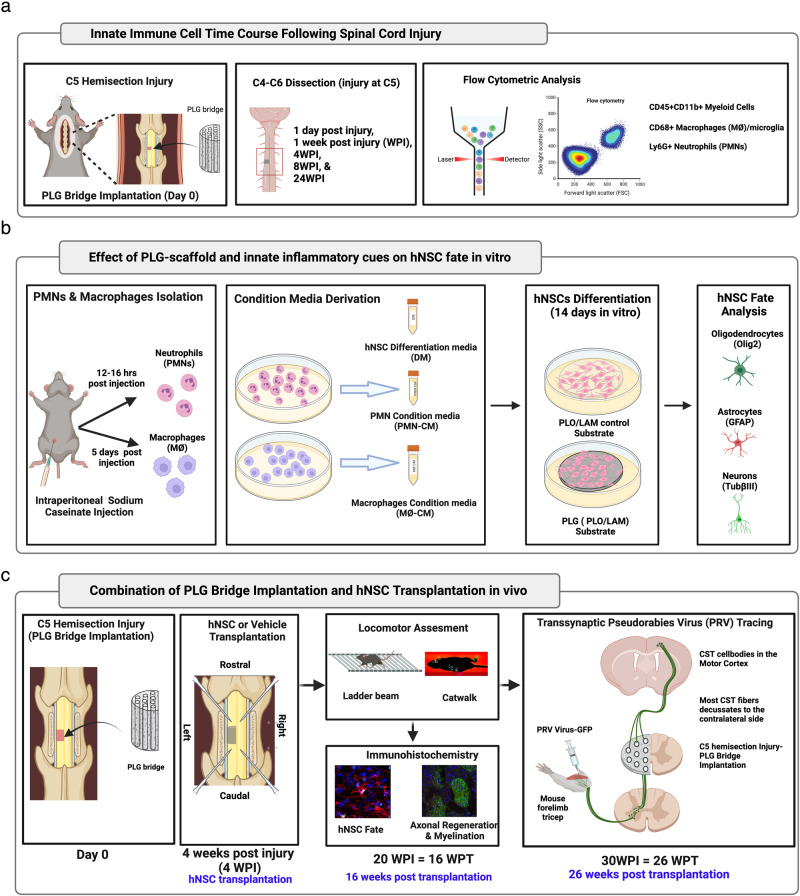
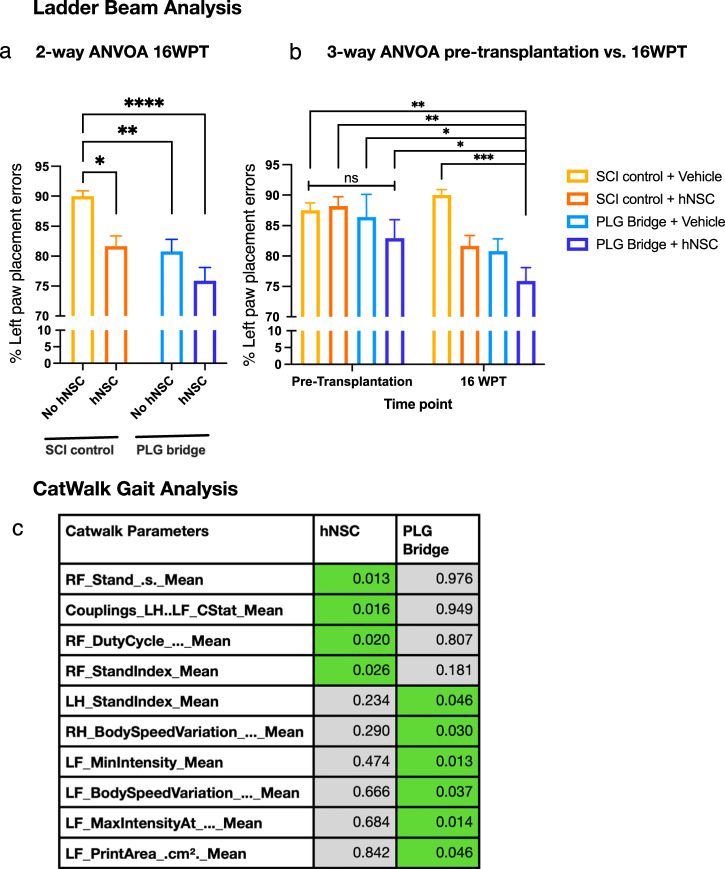
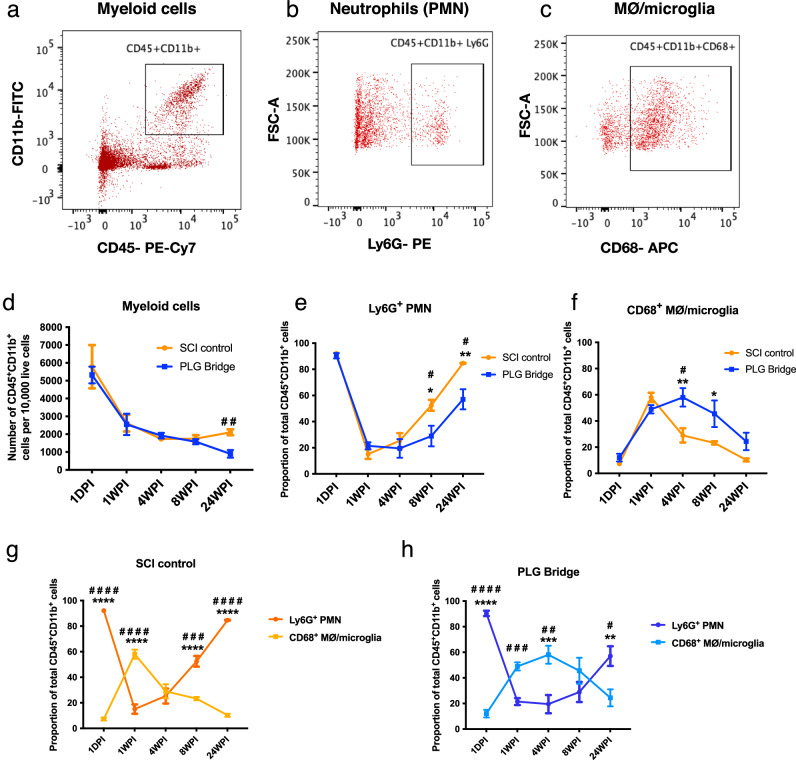
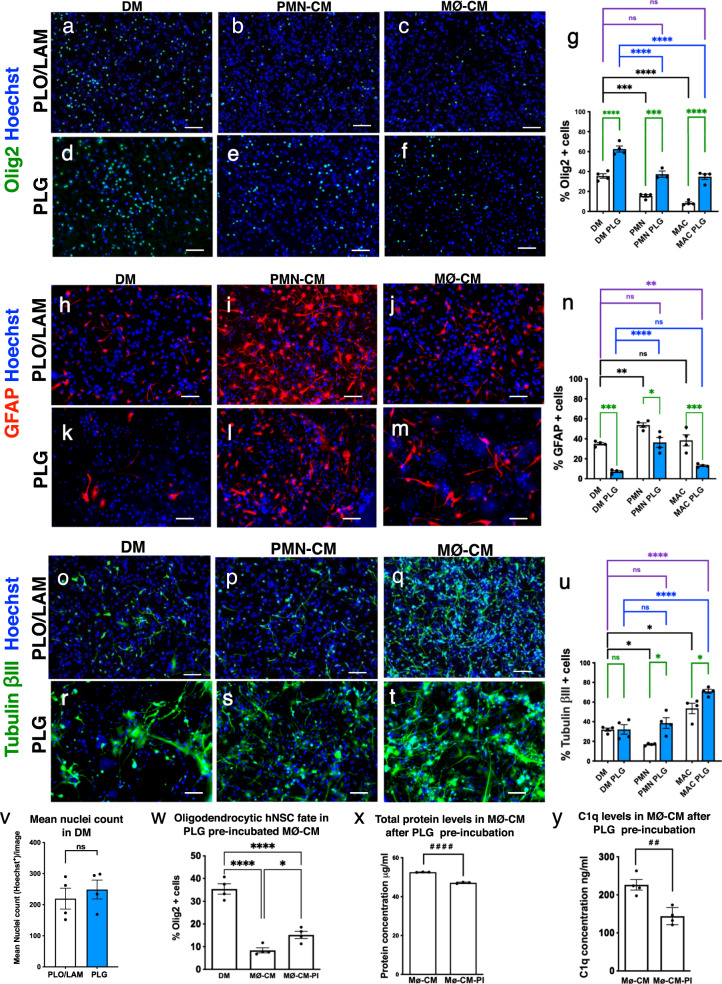
Regeneration in the injured spinal cord is limited by physical and chemical barriers. Acute implantation of a multichannel poly(lactide-co-glycolide) (PLG) bridge mechanically stabilizes the injury, modulates inflammation, and provides a permissive environment for rapid cellularization and robust axonal regrowth through this otherwise inhibitory milieu. However, without additional intervention, regenerated axons remain largely unmyelinated (<10%), limiting functional repair. While transplanted human neural stem cells (hNSC) myelinate axons after spinal cord injury (SCI), hNSC fate is highly influenced by the SCI inflammatory microenvironment, also limiting functional repair. Accordingly, we investigated the combination of PLG scaffold bridges with hNSC to improve histological and functional outcome after SCI. In vitro, hNSC culture on a PLG scaffold increased oligodendroglial lineage selection after inflammatory challenge. In vivo, acute PLG bridge implantation followed by chronic hNSC transplantation demonstrated a robust capacity of donor human cells to migrate into PLG bridge channels along regenerating axons and integrate into the host spinal cord as myelinating oligodendrocytes and synaptically integrated neurons. Axons that regenerated through the PLG bridge formed synaptic circuits that connected the ipsilateral forelimb muscle to contralateral motor cortex. hNSC transplantation significantly enhanced the total number of regenerating and myelinated axons identified within the PLG bridge. Finally, the combination of acute bridge implantation and hNSC transplantation exhibited robust improvement in locomotor recovery. These data identify a successful strategy to enhance neurorepair through a temporally layered approach using acute bridge implantation and chronic cell transplantation to spare tissue, promote regeneration, and maximize the function of new axonal connections.
脊髓损伤后的再生受到物理和化学屏障的限制。急性植入多通道聚乳酸-乙醇酸共聚物(PLG)桥可机械稳定损伤部位,调节炎症反应,并为细胞快速聚集和轴突在原本具有抑制性的环境中强劲再生提供有利环境。然而,若无额外干预,再生轴突大多仍未髓鞘化(<10%),限制了功能修复。虽然移植的人神经干细胞(hNSC)在脊髓损伤(SCI)后可使轴突髓鞘化,但hNSC的命运受SCI炎症微环境的高度影响,这也限制了功能修复。因此,我们研究了PLG支架桥与hNSC的联合应用,以改善SCI后的组织学和功能结果。在体外,在PLG支架上培养hNSC可增加炎症刺激后的少突胶质细胞谱系选择。在体内,急性植入PLG桥后进行慢性hNSC移植表明,供体人类细胞具有强大的能力,可沿再生轴突迁移至PLG桥通道,并作为髓鞘化少突胶质细胞和突触整合神经元融入宿主脊髓。通过PLG桥再生的轴突形成了连接同侧前肢肌肉与对侧运动皮层的突触回路。hNSC移植显著增加了PLG桥内再生和髓鞘化轴突的总数。最后,急性桥植入与hNSC移植的联合应用在运动恢复方面表现出显著改善。这些数据确定了一种成功的策略,即通过使用急性桥植入和慢性细胞移植的时间分层方法来增强神经修复,以保留组织、促进再生并最大化新轴突连接的功能。