Department of Anesthesia and Intensive Care, Næstved-Slagelse-Ringsted, Slagelse Hospital, Slagelse, Denmark.
Department of Anaesthesia and Intensive Care, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark.
Vasc Health Risk Manag. 2024 Mar 14;20:125-140. doi: 10.2147/VHRM.S427211. eCollection 2024.
The prevalence of occlusive lower extremity artery disease (LEAD) is rising worldwide while European epidemiology data are scarce. We report incidence and mortality of LEAD repair in Denmark from 1996 through 2018, stratified on open aorto-iliac, open peripheral, and endovascular repair.
A nationwide cohort study of prospective data from population-based Danish registers covering 1996 to 2018. Comorbidity was assessed by Charlson's Comorbidity Index (CCI). Incidence rate (IR) ratios and mortality rate ratios (MRR) were estimated by multivariable Poisson and Cox regression, respectively.
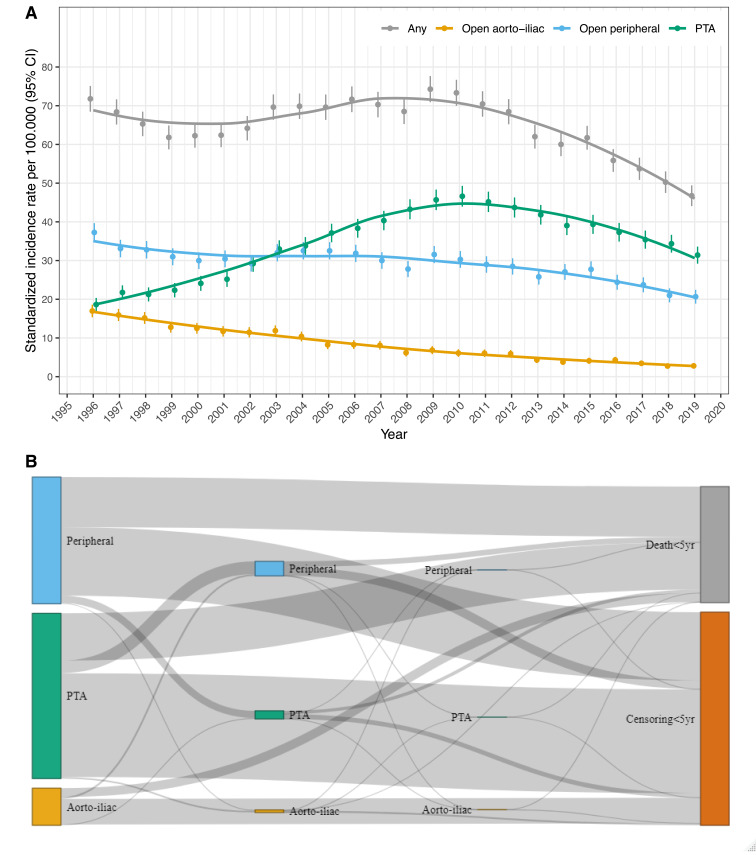
We identified 41,438 unique patients undergoing 46,236 incident first-time LEAD repairs by either aorto-iliac- (n=5213), peripheral surgery (n=18,665) or percutaneous transluminal angioplasty (PTA, n=22,358). From 1996 to 2018, the age- and sex-standardized IR for primary revascularization declined from 71.8 to 50.2 per 100,000 person-years (IRR, 0.70; 95% CI, 0.66-0.75). Following a 2.5-fold IR increase of PTA from 1996 to 2010, all three repair techniques showed a declining trend after 2010. The declining IR was driven by decreasing LEAD repair due to claudication, and by persons aged below 80 years, while the IR increased in persons aged above 80 years (p interaction<0.001). LEAD repair was more frequent in men (IRR, 0.78; 95% CI, 0.77-0.80), which was consistent over calendar time (p interaction=0.41). Crude mortality decreased following open/surgical repair, and increased following PTA, but all three techniques trended towards lower adjusted mortality comparing the start and the end of the study period (MRR, 0.71; 95% CI, 0.54-0.93 vs MRR, 0.76; 95% CI, 0.69-0.83 vs MRR, 0.96; 95% CI, 0.86-1.07). Increasing age and CCI, male sex, smoking, and care dependency associated with increased mortality.
The incidence rate of LEAD repair decreased in Denmark from 1996 to 2018, especially in persons younger than 80 years, and primarily due to reduced revascularization for claudication. Adjusted mortality rates decreased following open surgery, but seemed unaltered following PTA.
阻塞性下肢动脉疾病(LEAD)的患病率在全球范围内呈上升趋势,而欧洲的流行病学数据却很少。我们报告了丹麦 1996 年至 2018 年期间行 LEAD 修复术的发病率和死亡率,按开放腹主动脉-髂动脉、开放外周血管和血管内修复术分层。
这是一项基于人群的全国性队列研究,对丹麦登记处的前瞻性数据进行了分析,时间范围为 1996 年至 2018 年。采用 Charlson 合并症指数(CCI)评估合并症。采用多变量泊松和 Cox 回归分别估计发病率(IR)比和死亡率(MRR)。
我们确定了 41438 名首次接受腹主动脉-髂动脉(n=5213)、外周手术(n=18665)或经皮腔内血管成形术(PTA,n=22358)的初次 LEAD 修复术的患者。1996 年至 2018 年,原发性血运重建的年龄和性别标准化发病率从 71.8 降至 50.2/100000 人年(IRR,0.70;95%CI,0.66-0.75)。1996 年至 2010 年,PTA 的发病率增加了 2.5 倍,此后三种修复技术均呈下降趋势。下降的发病率是由于跛行导致的 LEAD 修复减少,以及 80 岁以下人群减少所致,而 80 岁以上人群的发病率则增加(p 交互<0.001)。男性 LEAD 修复术更常见(IRR,0.78;95%CI,0.77-0.80),且这种趋势在整个时间范围内都一致(p 交互=0.41)。与研究开始和结束时相比,开放/手术修复后的死亡率降低,而 PTA 后死亡率增加(MRR,0.71;95%CI,0.54-0.93 vs MRR,0.76;95%CI,0.69-0.83 vs MRR,0.96;95%CI,0.86-1.07)。年龄和 CCI 增加、男性、吸烟和依赖护理与死亡率增加相关。
1996 年至 2018 年,丹麦 LEAD 修复术的发病率下降,尤其是 80 岁以下人群,主要原因是跛行患者的血运重建减少。开放手术后的调整死亡率降低,但 PTA 后似乎没有改变。