Centro de Investigaciones Endocrinológicas "Dr. César Bergadá" (CEDIE), CONICET - FEI - División de Endocrinología, Hospital de Niños Ricardo Gutiérrez, Buenos Aires, Argentina.
Universidad de Buenos Aires, Facultad de Medicina, Departamento de Biología Celular, Histología, Embriología y Genética, Buenos Aires, Argentina.
Front Endocrinol (Lausanne). 2024 Mar 4;15:1361032. doi: 10.3389/fendo.2024.1361032. eCollection 2024.
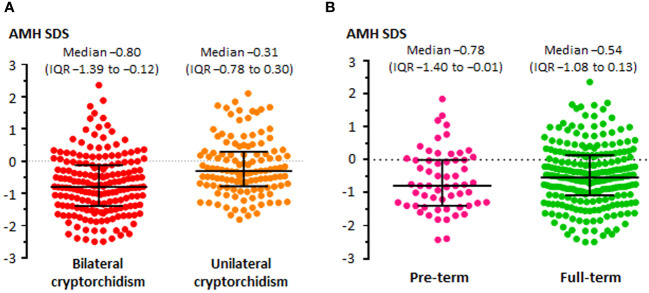
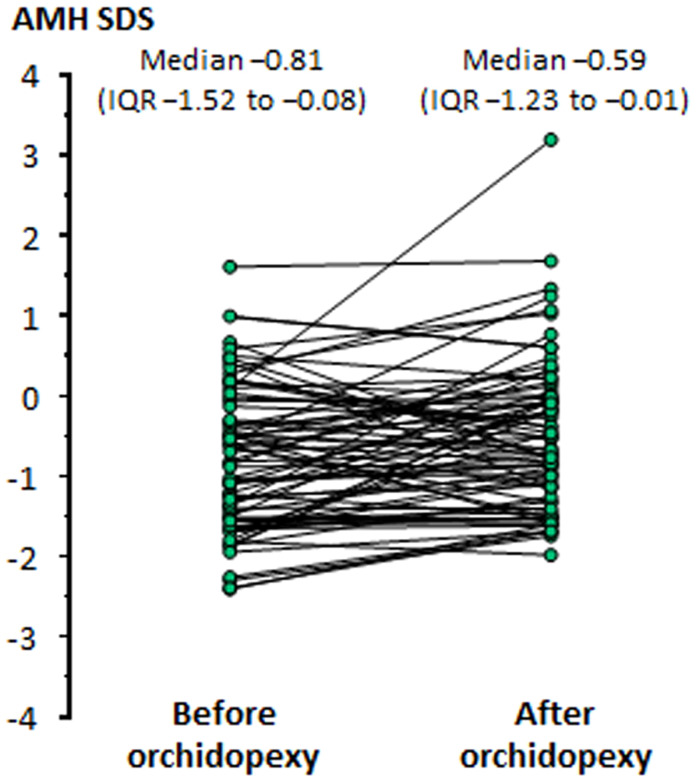
Anti-Müllerian hormone (AMH) is a Sertoli cell-secreted glycoprotein involved in male fetal sex differentiation: it provokes the regression of Müllerian ducts, which otherwise give rise to the Fallopian tubes, the uterus and the upper part of the vagina. In the first trimester of fetal life, AMH is expressed independently of gonadotropins, whereas from the second trimester onwards AMH testicular production is stimulated by FSH and oestrogens; at puberty, AMH expression is inhibited by androgens. AMH has also been suggested to participate in testicular descent during fetal life, but its role remains unclear. Serum AMH is a well-recognized biomarker of testicular function from birth to the first stages of puberty. Especially in boys with nonpalpable gonads, serum AMH is the most useful marker of the existence of testicular tissue. In boys with cryptorchidism, serum AMH levels reflect the mass of functional Sertoli cells: they are lower in patients with bilateral than in those with unilateral cryptorchidism. Interestingly, serum AMH increases after testis relocation to the scrotum, suggesting that the ectopic position result in testicular dysfunction, which may be at least partially reversible. In boys with cryptorchidism associated with micropenis, low AMH and FSH are indicative of central hypogonadism, and serum AMH is a good marker of effective FSH treatment. In patients with cryptorchidism in the context of disorders of sex development, low serum AMH is suggestive of gonadal dysgenesis, whereas normal or high AMH is found in patients with isolated androgen synthesis defects or with androgen insensitivity. In syndromic disorders, assessment of serum AMH has shown that Sertoli cell function is preserved in boys with Klinefelter syndrome until mid-puberty, while it is affected in patients with Noonan, Prader-Willi or Down syndromes.
抗缪勒管激素(AMH)是一种由支持细胞分泌的糖蛋白,参与男性胎儿性别分化:它促使缪勒管退化,否则缪勒管会发育成输卵管、子宫和阴道上段。在胎儿生命的第一个 trimester,AMH 的表达独立于促性腺激素,而从第二个 trimester 开始,FSH 和雌激素刺激睾丸产生 AMH;在青春期,雄激素抑制 AMH 的表达。AMH 也被认为参与胎儿期睾丸下降,但作用尚不清楚。血清 AMH 是从出生到青春期早期睾丸功能的公认生物标志物。特别是在无法触及性腺的男孩中,血清 AMH 是存在睾丸组织的最有用标志物。在隐睾症男孩中,血清 AMH 水平反映功能性支持细胞的数量:双侧隐睾症患者的水平低于单侧隐睾症患者。有趣的是,睾丸移位至阴囊后血清 AMH 水平升高,提示异位导致睾丸功能障碍,至少部分是可逆的。在伴有小阴茎的隐睾症男孩中,低 AMH 和 FSH 提示中枢性性腺功能减退,血清 AMH 是 FSH 有效治疗的良好标志物。在伴有性发育障碍的隐睾症患者中,低血清 AMH 提示性腺发育不良,而孤立的雄激素合成缺陷或雄激素不敏感患者中发现正常或高 AMH。在综合征性疾病中,血清 AMH 评估表明,Klinefelter 综合征男孩的支持细胞功能在青春期中期前保持正常,而 Noonan、Prader-Willi 或 Down 综合征患者的支持细胞功能受到影响。