Bonù Marco Lorenzo, Magli Alessandro, Tomasini Davide, Frassine Francesco, Albano Domenico, Arcangeli Stefano, Bruni Alessio, Ciccarelli Stefano, De Angeli Martina, Francolini Giulio, Franzese Ciro, Ghirardelli Paolo, Grazioli Luigi, Guerini Andrea, Lancia Andrea, Marvaso Giulia, Sepulcri Matteo, Trodella Luca Eolo, Morelli Vittorio, Georgopulos Andrea, Domina Anastasiya Oleksandrivna, Granello Lorenzo, Mataj Eneida, Barbera Fernando, Triggiani Luca
Department of Radiation Oncology, Istituto del Radio O.Alberti, University of Brescia and Spedali Civili Hospital, Brescia, Italy.
Department of Radiation Oncology, AULSS 1 Belluno, Belluno, Italy.
BJR Open. 2022 Nov 29;4(1):20220032. doi: 10.1259/bjro.20220032. eCollection 2022.
The therapeutic landscape for localized prostate cancer (PC) is evolving. Stereotactic radiotherapy (SRT) has been reported to be at least not inferior to standard radiotherapy, but the effect of androgen deprivation therapy (ADT) in this setting is still unknown and its use is left to clinical judgment. There is therefore the need to clarify the role of ADT in association with SRT, which is the aim of the present study.
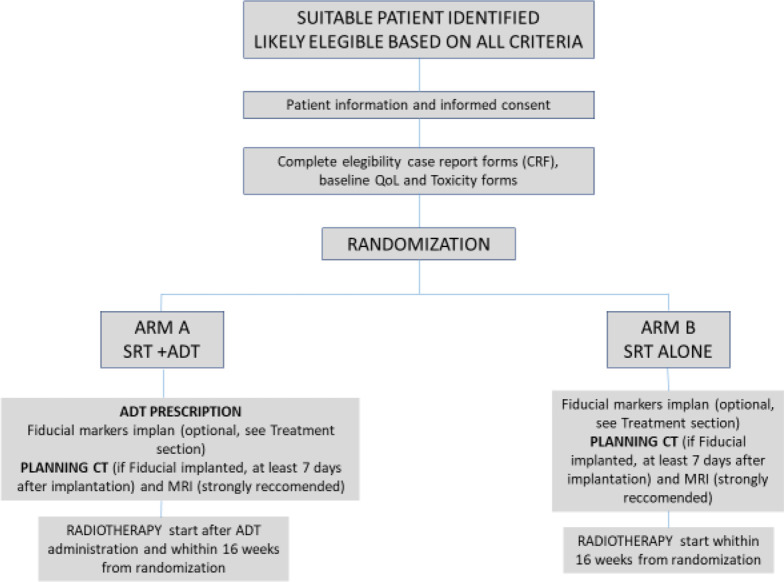
We present a study protocol for a randomized, multi-institutional, Phase III clinical trial, designed to study SRT in unfavorable intermediate and a subclass of high-risk localized PC. Patients (pts) will be randomized 1:1 to SRT + ADT or SRT alone. SRT will consists in 36.25 Gy in 5 fractions, ADT will be a single administration of Triptorelin 22.5 mg concurrent to SRT. Primary end point will be biochemical disease-free survival. Secondary end points will be disease-free survival, freedom from local recurrence, freedom from regional recurrence, freedom from distant metastasis and overall survival (OS); quality of life QoL and patient reported outcomes will be an exploratory end point and will be scored with EPIC-26, EORTC PR 25, IPSS, IIEF questionnaires in SRT + ADT and SRT alone arms. Moreover, clinician reported acute and late toxicity, assessed with CTCAE v. 5.0 scales will be safety end points.
Sample size is estimated of 310 pts. For acute toxicity and quality of life results are awaited after 6 months since last patient in, whereas, for efficacy end points and late toxicity mature results will be available 3-5 years after last patient in.
Evidence is insufficient to guide decision making concerning ADT administration in the new scenario of prostate ultra-hypofractionation. Hence, the need to investigate the ADT role in SRT specific setting.
The stereotactic prostate radiotherapy with or without ADT trial (SPA Trial) has been designed to establish a new standard of care for SRT in localized unfavorable intermediate and a subclass of localized high risk PC.
局限性前列腺癌(PC)的治疗格局正在不断演变。据报道,立体定向放射治疗(SRT)至少不逊色于标准放疗,但雄激素剥夺治疗(ADT)在此情况下的效果仍不明确,其使用需临床判断。因此,有必要阐明ADT联合SRT的作用,这也是本研究的目的。
我们提出了一项随机、多机构、III期临床试验的研究方案,旨在研究SRT用于预后不良的中危和高危局限性PC的一个亚类。患者将按1:1随机分为SRT + ADT组或单纯SRT组。SRT将采用5次分割共36.25 Gy,ADT将在SRT同时单次给予曲普瑞林22.5 mg。主要终点将是生化无病生存期。次要终点将是无病生存期、局部复发率、区域复发率、远处转移率和总生存期(OS);生活质量(QoL)和患者报告结局将作为探索性终点,并在SRT + ADT组和单纯SRT组中使用EPIC - 26、EORTC PR 25、IPSS、IIEF问卷进行评分。此外,使用CTCAE v. 5.0量表评估的临床医生报告的急性和晚期毒性将作为安全性终点。
估计样本量为310例患者。对于急性毒性和生活质量,自最后一名患者入组6个月后等待结果,而对于疗效终点和晚期毒性,在最后一名患者入组3 - 5年后将获得成熟结果。
在前列腺超分割的新情况下,证据不足以指导关于ADT给药的决策。因此,需要研究ADT在SRT特定环境中的作用。
立体定向前列腺放疗联合或不联合ADT试验(SPA试验)旨在为局限性预后不良的中危和局限性高危PC的一个亚类建立SRT的新护理标准。