Department of Diagnostic and Interventional Neuroradiology, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse, 3010, Bern, Switzerland.
Department of Neuroradiology, Clinic for Radiology and Nuclear Medicine, University Hospital Basel, Petersgraben 4/Spitalstrasse 21, 4031, Basel, Switzerland.
Clin Neuroradiol. 2024 Sep;34(3):625-635. doi: 10.1007/s00062-024-01401-7. Epub 2024 Mar 25.
Flat-panel detector computed tomography (FDCT) is increasingly used in (neuro)interventional angiography suites. This study aimed to compare FDCT perfusion (FDCTP) with conventional multidetector computed tomography perfusion (MDCTP) in patients with acute ischemic stroke.
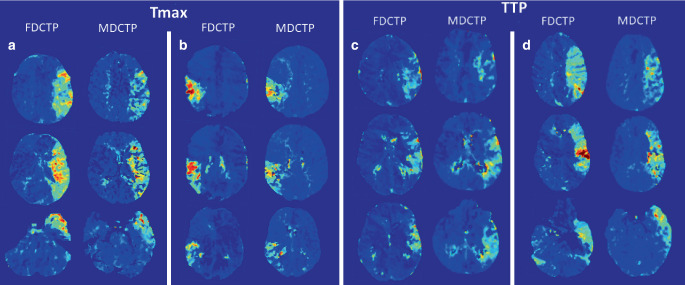
In this study, 19 patients with large vessel occlusion in the anterior circulation who had undergone mechanical thrombectomy, baseline MDCTP and pre-interventional FDCTP were included. Hypoperfused tissue volumes were manually segmented on time to maximum (Tmax) and time to peak (TTP) maps based on the maximum visible extent. Absolute and relative thresholds were applied to the maximum visible extent on Tmax and relative cerebral blood flow (rCBF) maps to delineate penumbra volumes and volumes with a high likelihood of irreversible infarcted tissue ("core"). Standard comparative metrics were used to evaluate the performance of FDCTP.
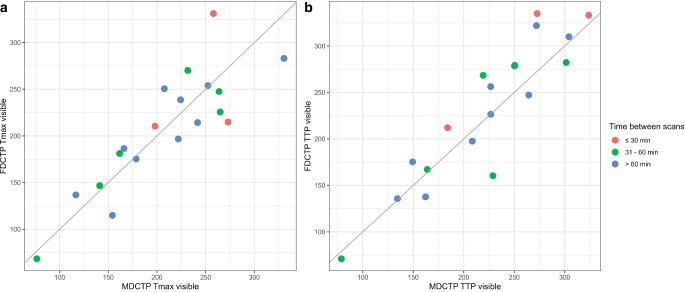
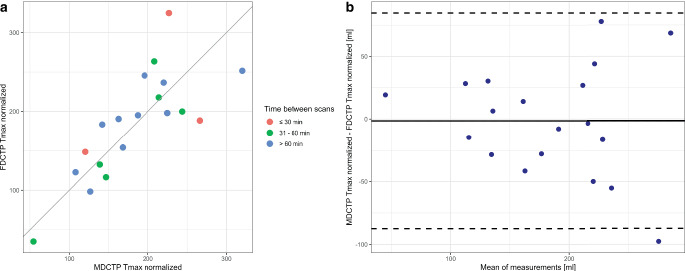
Strong correlations and robust agreement were found between manually segmented volumes on MDCTP and FDCTP Tmax maps (r = 0.85, 95% CI 0.65-0.94, p < 0.001; ICC = 0.85, 95% CI 0.69-0.94) and TTP maps (r = 0.91, 95% CI 0.78-0.97, p < 0.001; ICC = 0.90, 95% CI 0.78-0.96); however, direct quantitative comparisons using thresholding showed lower correlations and weaker agreement (MDCTP versus FDCTP Tmax 6 s: r = 0.35, 95% CI -0.13-0.69, p = 0.15; ICC = 0.32, 95% CI 0.07-0.75). Normalization techniques improved results for Tmax maps (r = 0.78, 95% CI 0.50-0.91, p < 0.001; ICC = 0.77, 95% CI 0.55-0.91). Bland-Altman analyses indicated a slight systematic underestimation of FDCTP Tmax maximum visible extent volumes and slight overestimation of FDCTP TTP maximum visible extent volumes compared to MDCTP.
FDCTP and MDCTP provide qualitatively comparable volumetric results on Tmax and TTP maps; however, direct quantitative measurements of infarct core and hypoperfused tissue volumes showed lower correlations and agreement.
平板探测器 CT(FDCT)在(神经)介入血管造影室中越来越多地被使用。本研究旨在比较急性缺血性卒中患者的 FDCT 灌注(FDCTP)与常规多层 CT 灌注(MDCTP)。
本研究纳入了 19 例接受机械血栓切除术的前循环大血管闭塞患者,进行了基线 MDCTP 和预介入 FDCTP。根据最大可见范围,在时间到最大值(Tmax)和时间到峰值(TTP)图上手动分割低灌注组织体积。在 Tmax 和相对脑血流量(rCBF)图上应用绝对和相对阈值来划定半暗带体积和高度可能不可逆梗死组织的体积(“核心”)。使用标准比较指标来评估 FDCTP 的性能。
MDCTP 和 FDCTP Tmax 图(r=0.85,95%CI 0.65-0.94,p<0.001;ICC=0.85,95%CI 0.69-0.94)和 TTP 图(r=0.91,95%CI 0.78-0.97,p<0.001;ICC=0.90,95%CI 0.78-0.96)之间存在较强的相关性和稳健的一致性;然而,使用阈值的直接定量比较显示出较低的相关性和较弱的一致性(MDCTP 与 FDCTP Tmax 6s:r=0.35,95%CI-0.13-0.69,p=0.15;ICC=0.32,95%CI 0.07-0.75)。Tmax 图的归一化技术改善了结果(r=0.78,95%CI 0.50-0.91,p<0.001;ICC=0.77,95%CI 0.55-0.91)。Bland-Altman 分析表明,与 MDCTP 相比,FDCTP Tmax 最大可见范围体积存在轻微的系统低估,FDCTP TTP 最大可见范围体积存在轻微的高估。
FDCTP 和 MDCTP 在 Tmax 和 TTP 图上提供了定性可比的容积结果;然而,对梗死核心和低灌注组织体积的直接定量测量显示出较低的相关性和一致性。