Panozzo Giacomo, Cicinelli Maria V, Dalla Mura Giulia, Giannarelli Diana, Vadalà Maria, Bonfiglio Vincenza, Bellisario Giovanni, Bandello Francesco
Ophthalmology Unit, Clinica San Francesco, Verona, Italy.
ESASO, European School of Advanced Studies in Ophthalmology, Lugano, Switzerland.
Ophthalmol Ther. 2024 May;13(5):1383-1398. doi: 10.1007/s40123-024-00925-y. Epub 2024 Mar 26.
This study assessed the European School of Advanced Studies in Ophthalmology (ESASO) classification's prognostic value for diabetic macular edema (DME) in predicting intravitreal therapy outcomes.
In this retrospective, multicenter study, patients aged > 50 years with type 1 or 2 diabetes and DME received intravitreal antivascular endothelial growth factor (anti-VEGF) agents (ranibizumab, bevacizumab, and aflibercept) or steroids (dexamethasone). The primary outcome was visual acuity (VA) change post-treatment, termed as functional response, measured 4-6 weeks post-third anti-VEGF or 12-16 weeks post-steroid injection, stratified by initial DME stage.
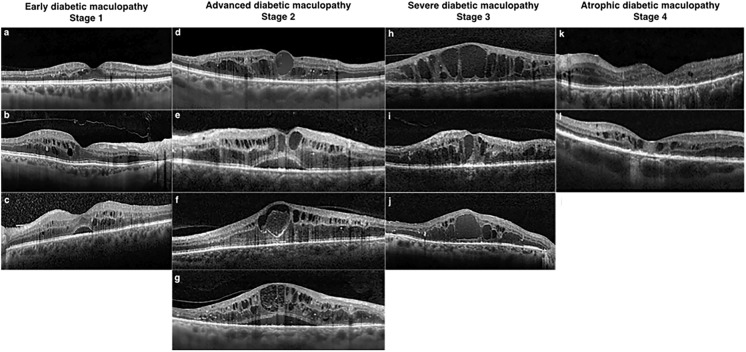
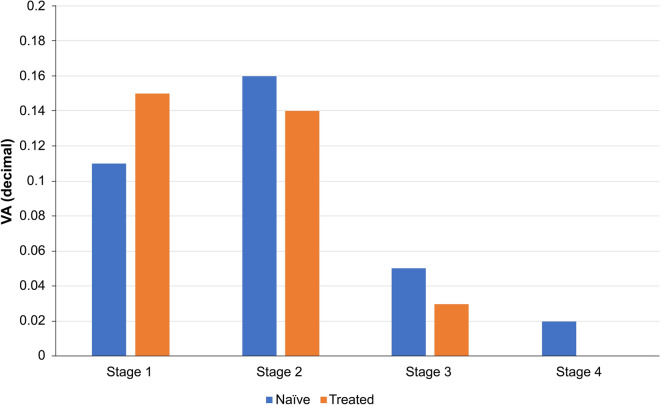
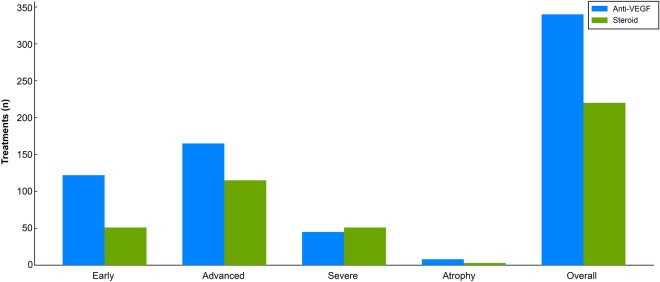
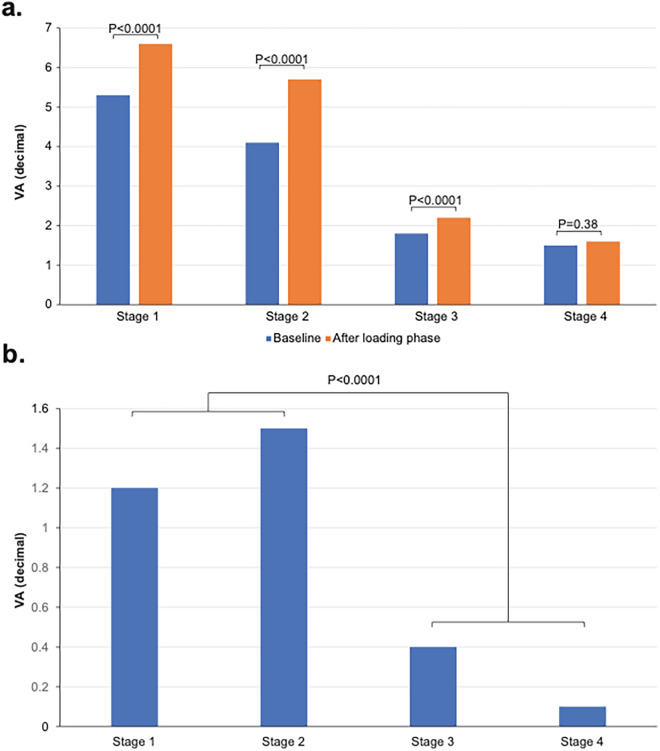
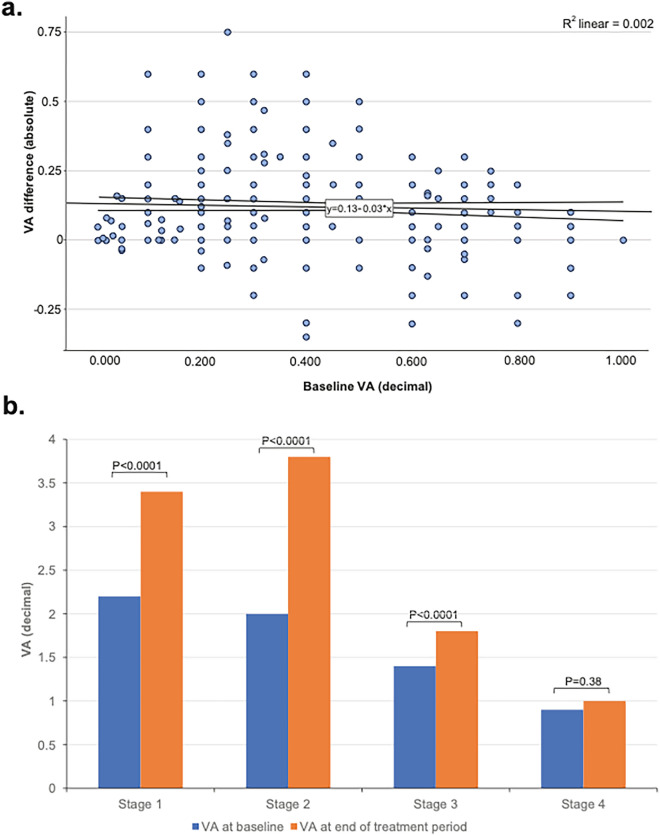
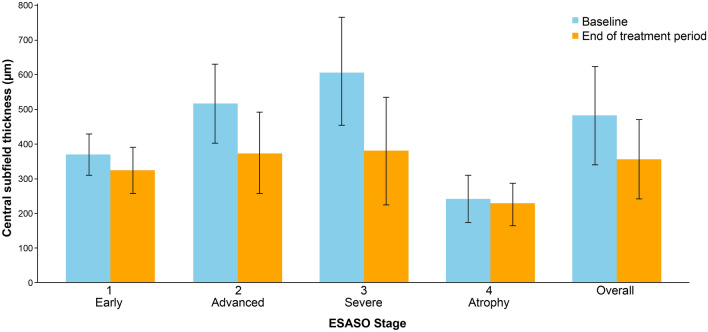
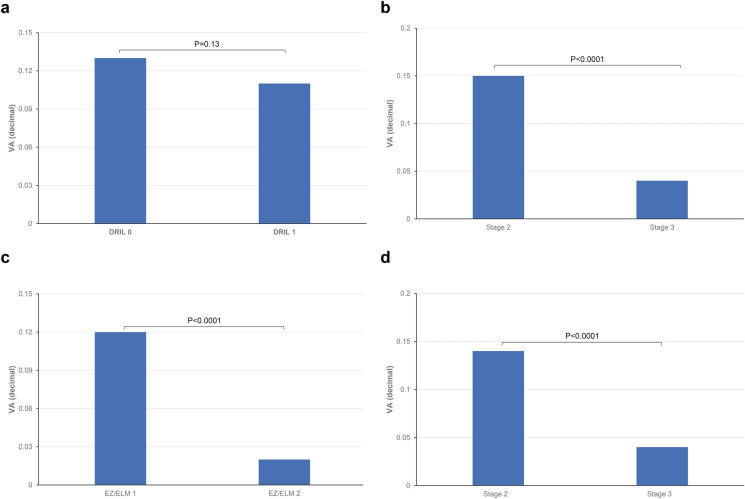
Of the 560 eyes studied (62% male, mean age 66.7 years), 31% were classified as stage 1 (early), 50% stage 2 (advanced), 17% stage 3 (severe), and 2% stage 4 (atrophic). Visual acuity (VA; decimal) improved by 0.12-0.15 decimals in stages 1-2 but only 0.03 decimal in stage 3 (all p < 0.0001) and 0.01 in stage 4 (p = 0.38). Even in eyes with low baseline VA ≤ 0.3, improvements were significant only in stages 1 and 2 (0.12 and 0.17 decimals, respectively). Central subfield thickness (CST) improvement was greatest in stage 3 (-229 µm, 37.6%, p < 0.0001), but uncorrelated with VA gains, unlike stages 1 and 2 (respectively: -142 µm, 27.4%; - 5 µm, 12%; both p < 0.0001). Stage 4 showed no significant CST change. Baseline disorganization of retinal inner layers and focal damage of the ellipsoid zone/external limiting membrane did not influence VA improvement in stages 1 and 2. Treatment patterns varied, with 61% receiving anti-VEGF and 39% dexamethasone, influenced by DME stage, with no significant differences between therapeutic agents.
The ESASO classification, which views the retina as a neurovascular unit and integrates multiple biomarkers, surpasses single biomarkers in predicting visual outcomes. Significant functional improvement occurred only in stages 1 and 2, suggesting reversible damage, whereas stages 3 and 4 likely reflect irreversible damage.
本研究评估了欧洲高级眼科学术院(ESASO)分类法对糖尿病性黄斑水肿(DME)预测玻璃体内治疗效果的预后价值。
在这项回顾性多中心研究中,年龄大于50岁的1型或2型糖尿病合并DME患者接受玻璃体内抗血管内皮生长因子(抗VEGF)药物(雷珠单抗、贝伐单抗和阿柏西普)或类固醇(地塞米松)治疗。主要结局是治疗后视力(VA)变化,即功能反应,在第三次抗VEGF治疗后4 - 6周或类固醇注射后12 - 16周测量,并按初始DME阶段分层。
在研究的560只眼中(62%为男性,平均年龄66.7岁),31%被分类为1期(早期),50%为2期(进展期),17%为3期(重度),2%为4期(萎缩期)。1 - 2期视力(VA;小数)提高了0.12 - 0.15,但3期仅提高了0.03(所有p < 0.0001),4期提高了0.01(p = 0.38)。即使在基线视力≤0.3的眼中,仅1期和2期有显著改善(分别为0.12和0.17)。中心子野厚度(CST)改善在3期最大(-229 µm,37.6%,p < 0.0001),但与视力提高无关,与1期和2期不同(分别为:-142 µm,27.4%;-5 µm,12%;均p < 0.0001)。4期CST无显著变化变化。视网膜内层的基线紊乱和椭圆体带/外界膜的局灶性损伤在1期和2期不影响视力改善。治疗模式各不相同,61%接受抗VEGF治疗,39%接受地塞米松治疗,受DME阶段影响,治疗药物之间无显著差异。
ESASO分类法将视网膜视为神经血管单元并整合多种生物标志物,在预测视力结果方面优于单一生物标志物。仅1期和2期有显著的功能改善,提示损伤可逆,而3期和4期可能反映不可逆损伤。