Cardiology, Department of Medical Sciences, University of Turin, Corso Dogliotti 14, 10126 Torino, Italy.
Division of Cardiology, Cardiovascular and Thoracic Department, 'Città della Salute e della Scienza' Hospital, Corso Bramante 88/90, 10126 Torino, Italy.
Europace. 2024 Mar 30;26(4). doi: 10.1093/europace/euae074.
Percutaneous stellate ganglion block (PSGB) through single-bolus injection and thoracic epidural anaesthesia (TEA) have been proposed for the acute management of refractory ventricular arrhythmias (VAs). However, data on continuous PSGB (C-PSGB) are scant. The aim of this study is to report our dual-centre experience with C-PSGB and to perform a systematic review on C-PSGB and TEA.
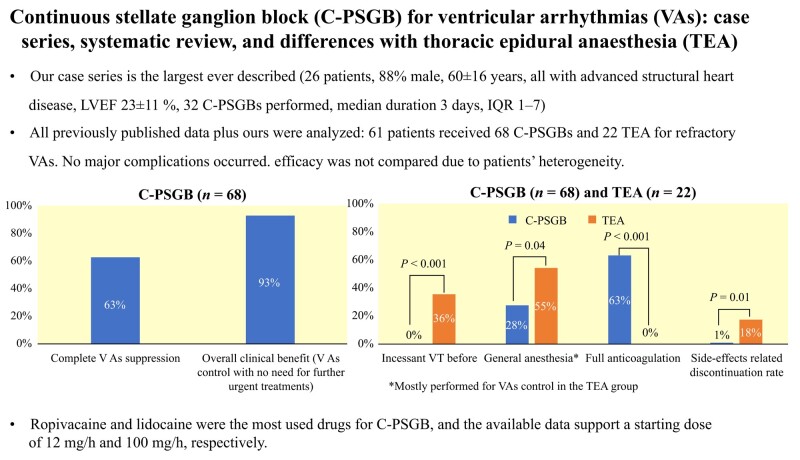
Consecutive patients receiving C-PSGB at two centres were enrolled. The systematic literature review follows the latest Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria. Our case series (26 patients, 88% male, 60 ± 16 years, all with advanced structural heart disease, left ventricular ejection fraction 23 ± 11%, 32 C-PSGBs performed, with a median duration of 3 days) shows that C-PSGB is feasible and safe and leads to complete VAs suppression in 59% and to overall clinical benefit in 94% of cases. Overall, 61 patients received 68 C-PSGBs and 22 TEA, with complete VA suppression in 63% of C-PSGBs (61% of patients). Most TEA procedures (55%) were performed on intubated patients, as opposed to 28% of C-PSGBs (P = 0.02); 63% of cases were on full anticoagulation at C-PSGB, none at TEA (P < 0.001). Ropivacaine and lidocaine were the most used drugs for C-PSGB, and the available data support a starting dose of 12 and 100 mg/h, respectively. No major complications occurred, yet TEA discontinuation rate due to side effects was higher than C-PSGB (18 vs. 1%, P = 0.01).
Continuous PSGB seems feasible, safe, and effective for the acute management of refractory VAs. The antiarrhythmic effect may be accomplished with less concerns for concomitant anticoagulation compared with TEA and with a lower side-effect related discontinuation rate.
经皮星状神经节阻滞(PSGB)单次注射和胸段硬膜外麻醉(TEA)已被提议用于治疗难治性室性心律失常(VA)的急性管理。然而,关于连续 PSGB(C-PSGB)的数据很少。本研究的目的是报告我们在两个中心使用 C-PSGB 的经验,并对 C-PSGB 和 TEA 进行系统评价。
连续在两个中心接受 C-PSGB 的患者被纳入研究。系统文献综述遵循最新的系统评价和荟萃分析(PRISMA)优先报告项目(PRISMA)标准。我们的病例系列(26 例患者,88%为男性,60±16 岁,均有晚期结构性心脏病,左心室射血分数 23±11%,行 32 次 C-PSGB,中位持续时间 3 天)表明 C-PSGB 是可行且安全的,可使 59%的患者完全抑制 VA,并使 94%的患者获得整体临床获益。总体而言,61 例患者接受了 68 次 C-PSGB 和 22 次 TEA,63%的 C-PSGB 完全抑制 VA(61%的患者)。大多数 TEA 操作(55%)是在气管插管的患者中进行的,而 C-PSGB 中只有 28%(P=0.02);C-PSGB 时 63%的病例接受了充分抗凝,而 TEA 时无抗凝(P<0.001)。罗哌卡因和利多卡因是 C-PSGB 最常用的药物,现有数据支持起始剂量分别为 12 和 100mg/h。没有发生重大并发症,但 TEA 因副作用而停止的发生率高于 C-PSGB(18%比 1%,P=0.01)。
连续 PSGB 似乎是可行、安全和有效的,可用于治疗难治性 VA 的急性发作。与 TEA 相比,抗心律失常作用可能在同时抗凝方面的顾虑更少,并且因副作用而停药的比例更低。