Thränhardt Pauline, Veselaj Admirim, Friedli Christoph, Wagner Franca, Marti Stefanie, Diem Lara, Hammer Helly, Radojewski Piotr, Wiest Roland, Chan Andrew, Hoepner Robert, Salmen Anke
Department of Neurology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Department of Neurology, Waikato Hospital, Hamilton, New Zealand.
Ther Adv Neurol Disord. 2024 Mar 26;17:17562864241237853. doi: 10.1177/17562864241237853. eCollection 2024.
Reporting of sex-specific analyses in multiple sclerosis (MS) is sparse. Disability accrual results from relapses (relapse-associated worsening) and independent thereof (progression independent of relapses).
A population of MS patients during relapse treated per standard of care was analyzed for sex differences and short-term relapse outcome (3-6 months) as measured by Expanded Disability Status Scale (EDSS) change.
Single-center retrospective study.
We analyzed 134 MS relapses between March 2016 and August 2020. All events required relapse treatment (steroids and/or plasma exchange). Demographic, disease, and paraclinical characteristics [cerebrospinal fluid (CSF) and magnetic resonance imaging (MRI)] were displayed separated by sex. Multivariable linear regression was run to identify factors associated with short-term EDSS change.
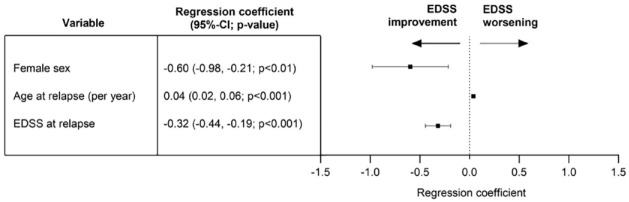
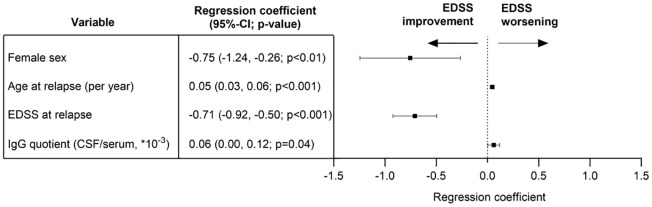
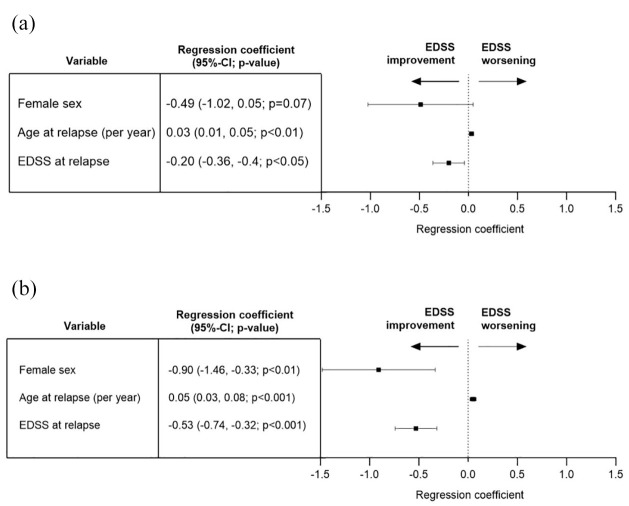
Mean age at relapse was 38.4 years (95% confidence interval: 36.3-40.4) with a proportion of 71.6% women in our cohort. Smoking was more than twice as prevalent in men (65.8%) than women (32.3%). In- and after-relapse EDSSs were higher in men [men: 3.3 (2.8-3.9), women: 2.7 (2.4-3.0); men: 3.0 (1.3-3.6); women: 1.8 (1.5-2.1)] despite similar relapse intervention. Paraclinical parameters revealed no sex differences. Our primary model identified female sex, younger age, and higher EDSS at relapse to be associated with EDSS improvement. A higher immunoglobulin G (IgG) quotient (CSF/serum) was associated with poorer short-term outcome [mean days between first relapse treatment and last EDSS assessment 130.2 (79.3-181.0)].
Sex and gender differences are important in outcome analyses of MS relapses. Effective treatment regimens need to respect putative markers for a worse outcome to modify long-term prognosis such as clinical and demographic variables, complemented by intrathecal IgG synthesis. Prospective trials should be designed to address these differences and confirm our results.
多发性硬化症(MS)中针对性别特异性分析的报告较少。残疾累积源于复发(与复发相关的病情恶化)及其独立因素(与复发无关的病情进展)。
分析按照标准治疗方案治疗的复发期MS患者群体的性别差异以及通过扩展残疾状态量表(EDSS)变化衡量的短期复发结局(3 - 6个月)。
单中心回顾性研究。
我们分析了2016年3月至2020年8月期间的134次MS复发。所有事件均需要进行复发治疗(使用类固醇和/或血浆置换)。人口统计学、疾病和辅助临床特征[脑脊液(CSF)和磁共振成像(MRI)]按性别分别展示。进行多变量线性回归以确定与短期EDSS变化相关的因素。
复发时的平均年龄为38.4岁(95%置信区间:36.3 - 40.4),我们队列中的女性比例为71.6%。男性吸烟率(65.8%)是女性(32.3%)的两倍多。尽管复发干预措施相似,但复发时及复发后的EDSS评分男性更高[男性:3.3(2.8 - 3.9),女性:2.7(2.4 - 3.0);男性:3.0(1.3 - 3.6);女性:1.8(1.5 - 2.1)]。辅助临床参数未显示出性别差异。我们的主要模型确定女性性别、较年轻的年龄以及复发时较高的EDSS与EDSS改善相关。较高的免疫球蛋白G(IgG)商(脑脊液/血清)与较差的短期结局相关[首次复发治疗与最后一次EDSS评估之间的平均天数为13,0.2(79.3 - 181.0)]。
性别差异在MS复发结局分析中很重要。有效的治疗方案需要考虑到提示较差结局的标志物,如临床和人口统计学变量,以及鞘内IgG合成,以改善长期预后。应设计前瞻性试验来研究这些差异并证实我们的结果。