Hospital for Special Surgery, New York, NY.
Weill Cornell Medical College, New York, NY.
Spine (Phila Pa 1976). 2024 Apr 15;49(8):561-568. doi: 10.1097/BRS.0000000000004714. Epub 2023 May 9.
Cross-sectional survey and retrospective review of prospectively collected data.
To explore how patients perceive their decision to pursue spine surgery for degenerative conditions and evaluate factors correlated with decisional regret.
Prior research shows that one-in-five older adults regret their decision to undergo spinal deformity surgery. However, no studies have investigated decisional regret in patients with degenerative conditions.
Patients who underwent cervical or lumbar spine surgery for degenerative conditions (decompression, fusion, or disk replacement) between April 2017 and December 2020 were included. The Ottawa Decisional Regret Questionnaire was implemented to assess prevalence of decisional regret. Questionnaire scores were used to categorize patients into low (<40) or medium/high (≥40) decisional regret cohorts. Patient-reported outcome measures (PROMs) included the Oswestry Disability Index, Patient-reported Outcomes Measurement Information System, Visual Analog Scale (VAS) Back/Leg/Arm, and Neck Disability Index at preoperative, early postoperative (<6 mo), and late postoperative (≥6 mo) timepoints. Differences in demographics, operative variables, and PROMs between low and medium/high decisional regret groups were evaluated.
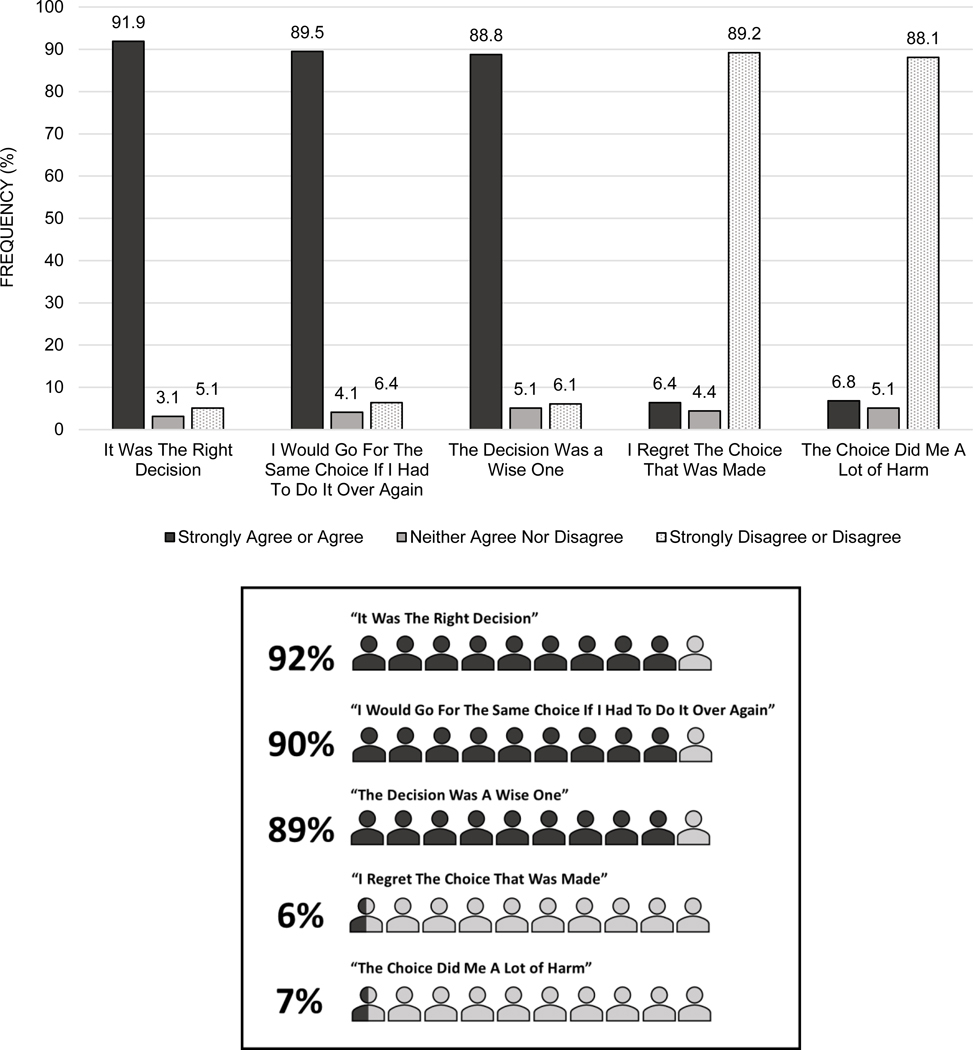
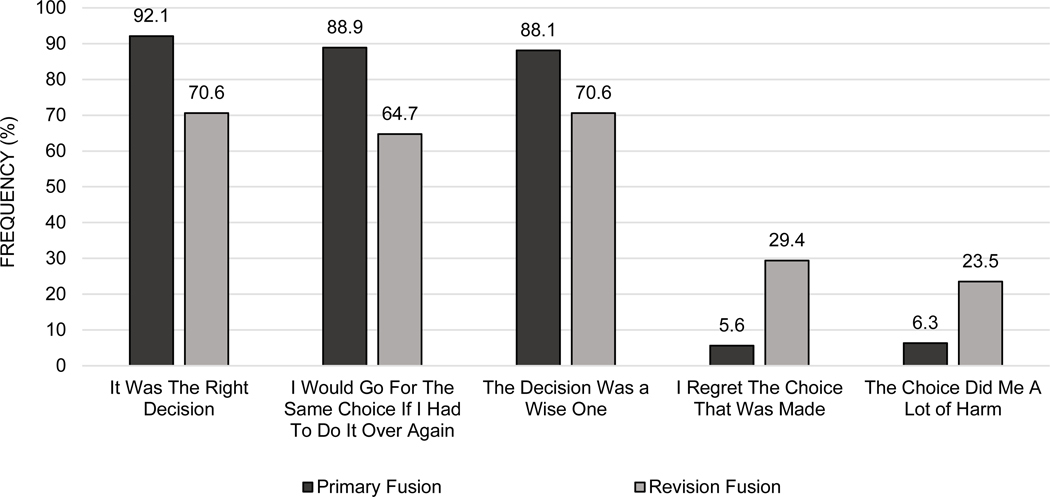
A total of 295 patients were included (mean follow-up: 18.2 mo). Overall, 92% of patients agreed that having surgery was the right decision, and 90% would make the same decision again. In contrast, 6% of patients regretted the decision to undergo surgery, and 7% noted that surgery caused them harm. In-hospital complications (P=0.02) and revision fusion (P=0.026) were significantly associated with higher regret. The medium/high decisional regret group also exhibited significantly worse PROMs at long-term follow-up for all metrics except VAS-Arm, and worse achievement of minimum clinically important difference for Oswestry Disability Index (P=0.007), Patient-Reported Outcomes Measurement Information System (P<0.0001), and VAS-Leg (P<0.0001).
Higher decisional regret was encountered in the setting of need for revision fusion, increased in-hospital complications, and worse PROMs. However, 90% of patients overall were satisfied with their decision to undergo spine surgery for degenerative conditions. Current tools for assessing patient improvement postoperatively may not adequately capture the psychosocial values and patient expectations implicated in decisional regret.
横断面调查和前瞻性数据回顾。
探讨患者对退行性疾病接受脊柱手术的决策的看法,并评估与决策后悔相关的因素。
先前的研究表明,五分之一的老年人对接受脊柱畸形手术的决定感到后悔。然而,尚无研究调查退行性疾病患者的决策后悔。
纳入 2017 年 4 月至 2020 年 12 月间因退行性疾病(减压、融合或椎间盘置换)接受颈椎或腰椎手术的患者。采用渥太华决策后悔问卷评估决策后悔的发生率。根据问卷评分将患者分为低(<40)或中/高(≥40)决策后悔组。患者报告的结果测量(PROM)包括 Oswestry 残疾指数、患者报告的结果测量信息系统、视觉模拟量表(VAS)背部/腿部/手臂和颈部残疾指数,术前、术后早期(<6 个月)和术后晚期(≥6 个月)。评估低和中/高决策后悔组之间的人口统计学、手术变量和 PROM 的差异。
共纳入 295 例患者(平均随访 18.2 个月)。总体而言,92%的患者认为手术是正确的决定,90%的患者会再次做出相同的决定。相比之下,6%的患者对手术决定感到后悔,7%的患者表示手术对他们造成了伤害。住院期间的并发症(P=0.02)和翻修融合(P=0.026)与较高的后悔显著相关。在长期随访中,中/高决策后悔组在除 VAS-手臂外的所有指标上的 PROM 均显著较差,Oswestry 残疾指数(P=0.007)、患者报告的结果测量信息系统(P<0.0001)和 VAS-腿部(P<0.0001)的最小临床重要差异的达标率也显著较差。
在需要翻修融合、住院并发症增加和 PROM 较差的情况下,决策后悔发生率较高。然而,总体而言,90%的患者对接受退行性疾病的脊柱手术感到满意。目前用于评估患者术后改善的工具可能无法充分捕捉到决策后悔所涉及的社会心理价值观和患者期望。