Division of Infectious Diseases, Duke University Medical Center, Durham, North Carolina.
Duke Center for Antimicrobial Stewardship and Infection Prevention, Durham, North Carolina.
JAMA Netw Open. 2024 Mar 4;7(3):e243846. doi: 10.1001/jamanetworkopen.2024.3846.
Despite modest reductions in the incidence of hospital-onset Clostridioides difficile infection (HO-CDI), CDI remains a leading cause of health care-associated infection. As no single intervention has proven highly effective on its own, a multifaceted approach to controlling HO-CDI is needed.
To assess the effectiveness of the Centers for Disease Control and Prevention's Strategies to Prevent Clostridioides difficile Infection in Acute Care Facilities Framework (hereafter, the Framework) in reducing HO-CDI incidence.
DESIGN, SETTING, AND PARTICIPANTS: This quality improvement study was performed within the Duke Infection Control Outreach Network from July 1, 2019, through March 31, 2022. In all, 20 hospitals in the network participated in an implementation study of the Framework recommendations, and 26 hospitals did not participate and served as controls. The Framework has 39 discrete intervention categories organized into 5 focal areas for CDI prevention: (1) isolation and contact precautions, (2) CDI confirmation, (3) environmental cleaning, (4) infrastructure development, and (5) antimicrobial stewardship engagement.
Monthly teleconferences supporting Framework implementation for the participating hospitals.
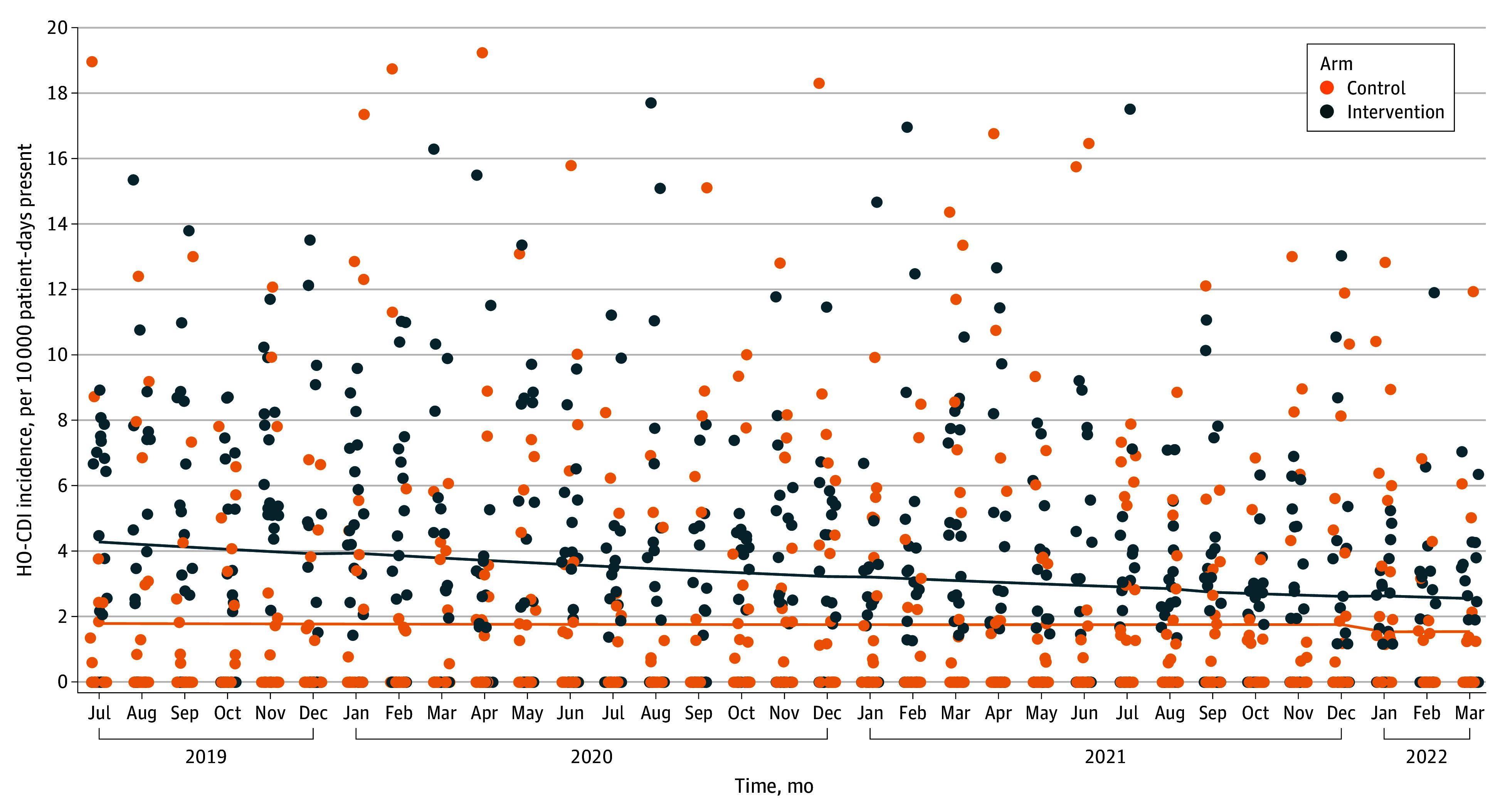
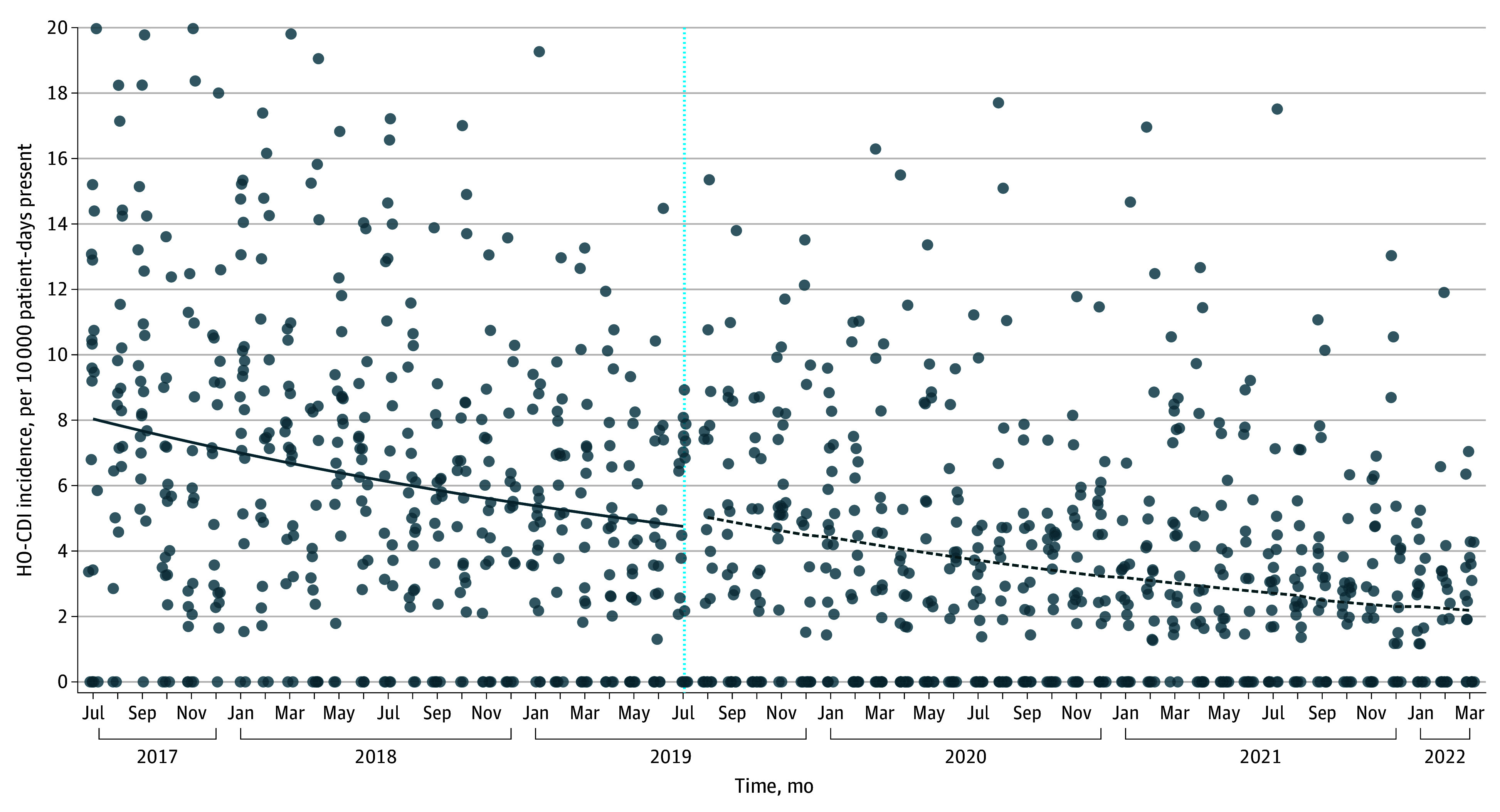
Primary outcomes were HO-CDI incidence trends at participating hospitals compared with controls and postintervention HO-CDI incidence at intervention sites compared with rates during the 24 months before the intervention.
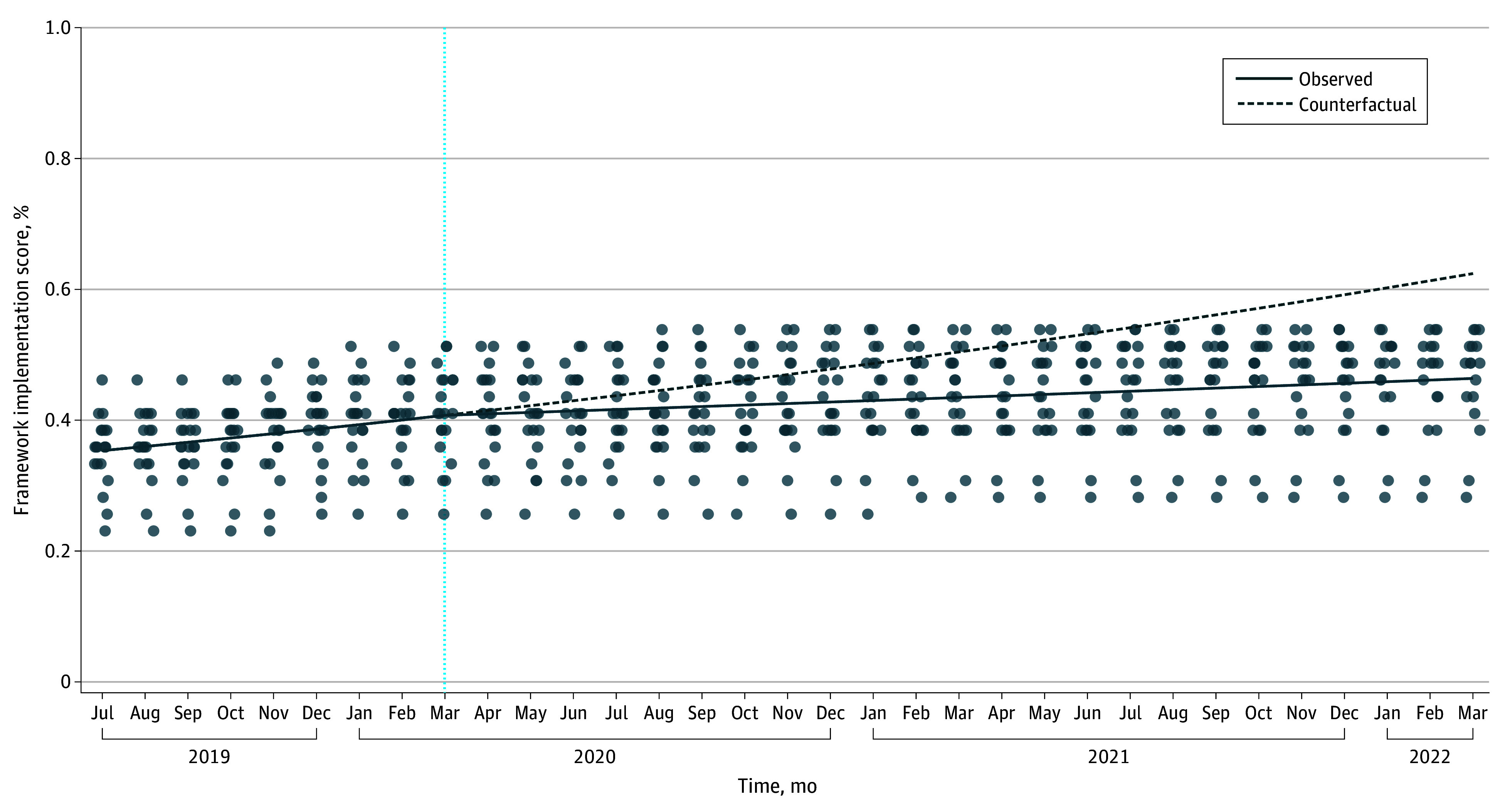
The study sample included a total of 2184 HO-CDI cases and 7 269 429 patient-days. In the intervention cohort of 20 participating hospitals, there were 1403 HO-CDI cases and 3 513 755 patient-days, with a median (IQR) HO-CDI incidence of 2.8 (2.0-4.3) cases per 10 000 patient-days. The first analysis included an additional 3 755 674 patient-days and 781 HO-CDI cases among the 26 controls, with a median (IQR) HO-CDI incidence of 1.1 (0.7-2.7) case per 10 000 patient-days. The second analysis included an additional 2 538 874 patient-days and 1751 HO-CDI cases, with a median (IQR) HO-CDI incidence of 5.9 (2.7-8.9) cases per 10 000 patient-days, from participating hospitals 24 months before the intervention. In the first analysis, intervention sites had a steeper decline in HO-CDI incidence over time relative to controls (yearly incidence rate ratio [IRR], 0.79 [95% CI, 0.67-0.94]; P = .01), but the decline was not temporally associated with study participation. In the second analysis, HO-CDI incidence was declining in participating hospitals before the intervention, and the rate of decline did not change during the intervention. The degree to which hospitals implemented the Framework was associated with steeper declines in HO-CDI incidence (yearly IRR, 0.95 [95% CI, 0.90-0.99]; P = .03).
In this quality improvement study of a regional hospital network, implementation of the Framework was not temporally associated with declining HO-CDI incidence. Further study of the effectiveness of multimodal prevention measures for controlling HO-CDI is warranted.
尽管医院获得性艰难梭菌感染 (HO-CDI) 的发病率有所下降,但 CDI 仍然是医疗保健相关感染的主要原因。由于没有单一的干预措施被证明非常有效,因此需要采取多方面的方法来控制 HO-CDI。
评估疾病控制与预防中心的策略对降低急性保健设施框架(以下简称框架)中 HO-CDI 发病率的有效性。
设计、地点和参与者:这项质量改进研究是在杜克感染控制外展网络内进行的,时间为 2019 年 7 月 1 日至 2022 年 3 月 31 日。该网络中的 20 家医院参与了框架建议的实施研究,26 家医院未参与并作为对照组。该框架有 39 个离散的干预类别,分为 5 个预防 CDI 的重点领域:(1)隔离和接触预防措施,(2)CDI 确认,(3)环境清洁,(4)基础设施开发,和(5)抗菌药物管理参与。
支持参与医院实施框架的每月电话会议。
主要结果是与对照组相比,参与医院的 HO-CDI 发病率趋势,以及干预点与干预前 24 个月期间的 HO-CDI 发病率相比。
研究样本包括共 2184 例 HO-CDI 病例和 7269429 名患者日。在 20 家参与医院的干预队列中,有 1403 例 HO-CDI 病例和 3513755 名患者日,中位数(IQR)HO-CDI 发病率为每 10000 名患者日 2.8(2.0-4.3)例。第一次分析包括对照组中另外 3755674 名患者日和 781 例 HO-CDI 病例,中位数(IQR)HO-CDI 发病率为每 10000 名患者日 1.1(0.7-2.7)例。第二次分析包括来自参与医院在干预前 24 个月的另外 2538874 名患者日和 1751 例 HO-CDI 病例,中位数(IQR)HO-CDI 发病率为每 10000 名患者日 5.9(2.7-8.9)例。在第一次分析中,与对照组相比,干预点的 HO-CDI 发病率随时间呈下降趋势(年发病率比[IRR],0.79[95%CI,0.67-0.94];P = .01),但下降趋势与研究参与无关。在第二次分析中,在干预之前,参与医院的 HO-CDI 发病率呈下降趋势,且在干预期间下降速度没有变化。医院实施框架的程度与 HO-CDI 发病率的大幅下降相关(年 IRR,0.95[95%CI,0.90-0.99];P = .03)。
在这项针对区域医院网络的质量改进研究中,框架的实施与 HO-CDI 发病率的下降没有时间上的关联。需要进一步研究控制 HO-CDI 的多模式预防措施的有效性。