Suzuki Shigeaki, Uzawa Akiyuki, Nagane Yuriko, Masuda Masayuki, Konno Shingo, Kubota Tomoya, Samukawa Makoto, Ishizuchi Kei, Tokuyasu Daiki, Handa Hideo, Yasuda Manato, Kawaguchi Naoki, Kimura Takashi, Suzuki Yasushi, Sugimoto Takamichi, Minami Naoya, Takahashi Masanori P, Murai Hiroyuki, Utsugisawa Kimiaki
Department of Neurology (SS, KI, DT), Keio University School of Medicine, Tokyo; Department of Neurology (AU, HH, MY), Graduate School of Medicine, Chiba University; Department of Neurology (YN, KU), Hanamaki General Hospital; Department of Neurology (MM), Tokyo Medical University; Department of Neurology (SK), Toho University Ohashi Medical Center, Tokyo; Division of Health Sciences (T. Kubota, MPT), Department of Clinical Laboratory and Biomedical Sciences, Osaka University Graduate School of Medicine; Department of Neurology (MS), Kindai University Faculty of Medicine, Sayama; Department of Neurology (NK), Neurology Chiba Clinic; Department of Neurology (T. Kimura), Hyogo Medical University, Nishinomiya; Department of Neurology (YS), National Hospital Organization Sendai Medical Center, Sendai; Department of Clinical Neuroscience and Therapeutics (TS), Hiroshima University; Department of Neurology (NM), National Hospital Organization Hokkaido Medical Center, Sapporo; and Department of Neurology (HM), International University of Health and Welfare, Narita, Japan.
Neurol Clin Pract. 2024 Jun;14(3):e200276. doi: 10.1212/CPJ.0000000000200276. Epub 2024 Mar 25.
Efgartigimod, which has been well tolerated and efficacious in individuals with generalized myasthenia gravis (MG), is available in Japan not only for the treatment of anti-acetylcholine receptor-positive (AChR+) but also anti-muscle-specific receptor tyrosine kinase (MuSK+) and seronegative generalized MG. We report details of the use of efgartigimod for generalized MG in clinical practice in Japan.
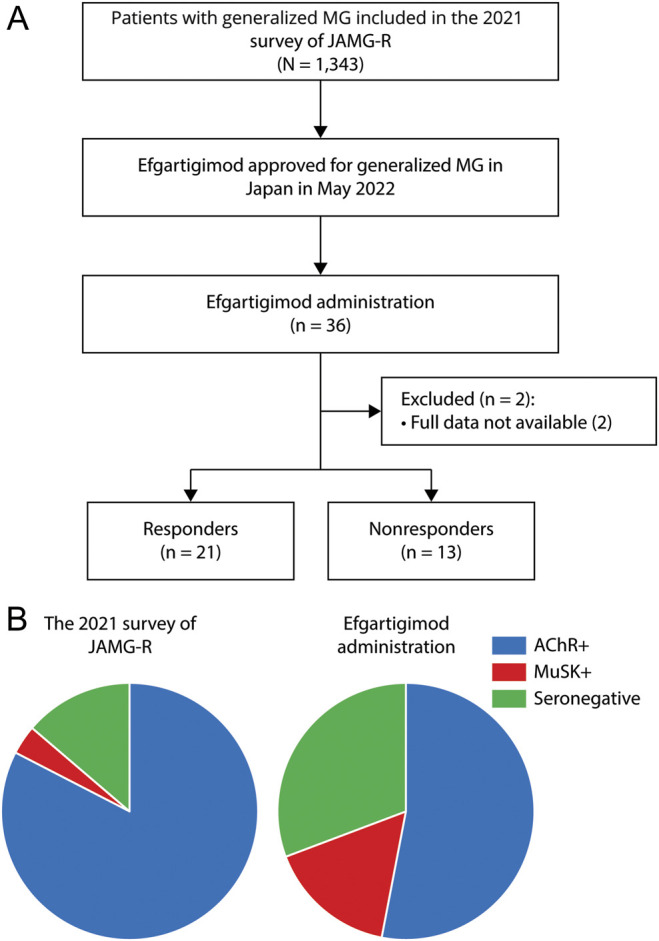
We included patients with generalized MG in the 2021 survey of Japan Myasthenia Gravis Registry (JAMG-R) study group who received an initial cycle of efgartigimod between May and September 2022. We defined "responders" as patients who achieved a score ≥2 points for MG activities of daily living (MG-ADL) in the first treatment cycle. The MG composite and the Revised scale of the 15-item Myasthenia Gravis-Quality of Life scale (MG-QOL15-r) were also evaluated.
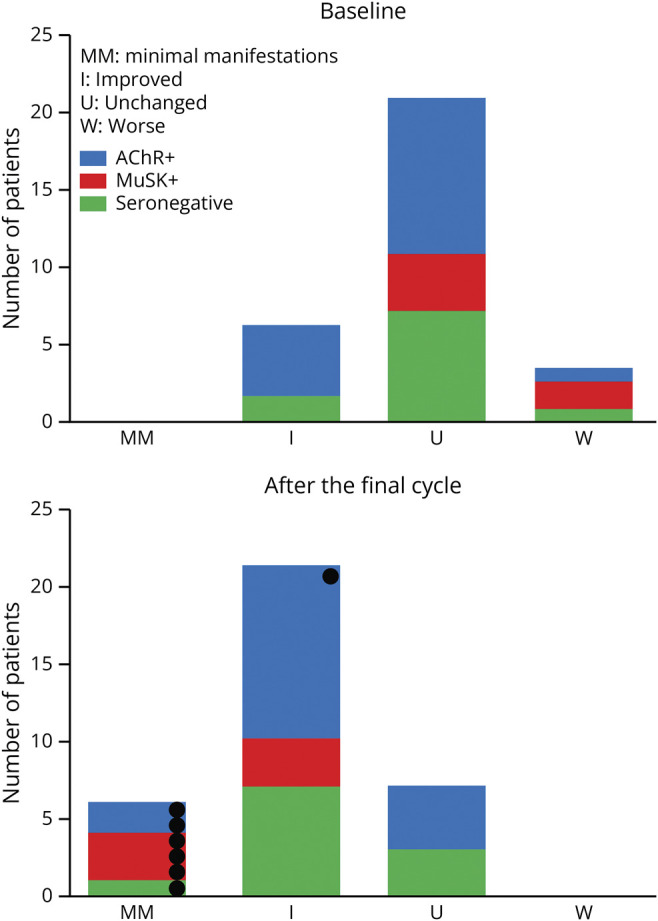
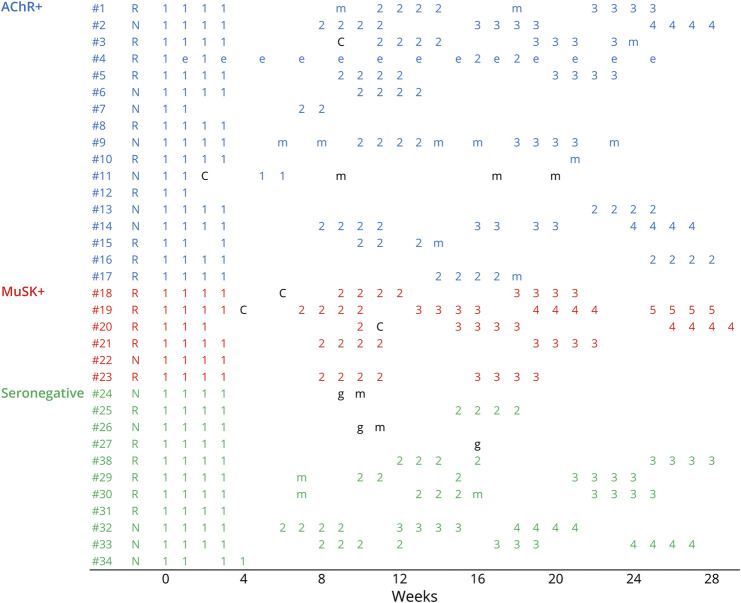
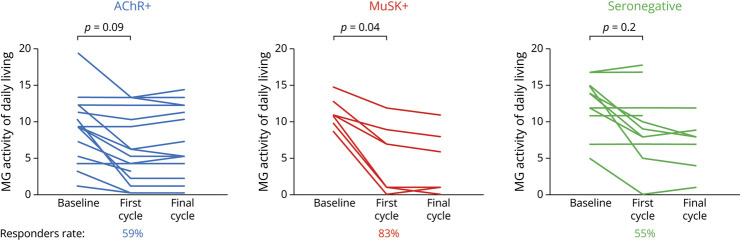
Of 1,343 JAMG-R patients, 36 (2.7%) started efgartigimod (female 68%, age 53 years). Their serologic profiles were as follows: AChR+, n = 19 (53%); MuSK+, n = 6 (17%); and seronegative, n = 11 (31%). Twenty-six patients (72%) had refractory MG. There were 81 cycles of efgartigimod during the 26-week observation in 34 patients (average, 2.4 cycles). The mean interval between cycles was 5.9 weeks. A continuous 4-weekly infusion of efgartigimod was performed in 65 (80%) of 81 cycles. In the first cycle, the MG-ADL score of the 34 patients decreased significantly from 10.5 ± 4.3 to 6.9 ± 5.1 ( = 0.003). Similarly, the mean MG composite and MG-QOL15-r decreased from 18.4 ± 13.6 to 11.8 ± 9.6 ( = 0.004) and from 19.2 ± 6.3 to 14.2 ± 8.3 ( = 0.007), respectively. Twenty-one (62%) patients were responders. Therapeutic responses were observed in the subsequent cycles. The duration of effectiveness of efgartigimod was varied among the responders; 4 responders had only a single effective cycle. Significant improvement was observed in the MuSK+ patients. Prednisolone dose of 7 patients was reduced. Our examination of the patients' postintervention status revealed that 6 patients achieved minimal manifestations. COVID-19 occurred in 5 patients. We failed to detect clinical or laboratory findings associated with responders.
Efgartigimod can be considered for the treatment of patients with generalized MG who do not achieve minimal manifestations, with a broad flexibility of patient selection and treatment schedules.
艾加莫德在全身性重症肌无力(MG)患者中耐受性良好且疗效显著,在日本不仅可用于治疗抗乙酰胆碱受体阳性(AChR+)的MG,还可用于治疗抗肌肉特异性受体酪氨酸激酶(MuSK+)和血清阴性全身性MG。我们报告了在日本临床实践中使用艾加莫德治疗全身性MG的详细情况。
我们纳入了2021年日本重症肌无力注册研究组(JAMG-R)研究中的全身性MG患者,这些患者在2022年5月至9月期间接受了艾加莫德的初始治疗周期。我们将“反应者”定义为在第一个治疗周期中MG日常生活活动(MG-ADL)评分≥2分的患者。还评估了MG综合评分和15项重症肌无力生活质量量表(MG-QOL15-r)的修订版。
在1343名JAMG-R患者中,36名(2.7%)开始使用艾加莫德(女性占68%,年龄53岁)。他们的血清学特征如下:AChR+,n = 19(53%);MuSK+,n = 6(17%);血清阴性,n = 11(31%)。26名患者(72%)患有难治性MG。在34名患者的26周观察期内进行了81个艾加莫德治疗周期(平均2.4个周期)。周期之间的平均间隔为5.9周。81个周期中的65个(80%)进行了连续4周一次的艾加莫德输注。在第一个周期中,34名患者的MG-ADL评分从10.5±4.3显著降至6.9±5.1(P = 0.003)。同样,MG综合评分和MG-QOL15-r的平均值分别从18.4±13.6降至11.8±9.6(P = 0.004)和从19.2±6.3降至14.2±8.3(P = 0.007)。21名(62%)患者为反应者。在随后的周期中观察到了治疗反应。艾加莫德的有效持续时间在反应者中各不相同;4名反应者只有一个有效周期。MuSK+患者有显著改善。7名患者的泼尼松剂量减少。我们对患者干预后状态的检查发现,6名患者达到了最小表现。5名患者发生了COVID-19。我们未能检测到与反应者相关的临床或实验室结果。
对于未达到最小表现的全身性MG患者,可考虑使用艾加莫德进行治疗,在患者选择和治疗方案方面具有广泛的灵活性。