Stanford Cancer Institute, Stanford University, Palo Alto, CA.
Royal North Shore Hospital, University of Sydney, St Leonards, Australia.
J Clin Oncol. 2024 Jul 10;42(20):2393-2403. doi: 10.1200/JCO.23.02166. Epub 2024 Mar 29.
Although checkpoint inhibitors have improved first-line treatment for non-small cell lung cancer (NSCLC), a therapeutic need remains for patients whose disease does not respond or who experience disease progression after anti-PD-L1/PD-1 immunotherapy. CONTACT-01 (ClinicalTrials.gov identifier: NCT04471428) evaluated atezolizumab plus cabozantinib versus docetaxel in patients with metastatic NSCLC who developed disease progression after concurrent or sequential treatment with anti-PD-L1/PD-1 and platinum-containing chemotherapy.
This multicenter, open-label, phase III trial randomly assigned patients 1:1 to atezolizumab 1,200 mg intravenously once every 3 weeks (q3w) plus cabozantinib 40 mg orally once daily or docetaxel 75 mg/m intravenously once every 3 weeks. The primary end point was overall survival (OS).
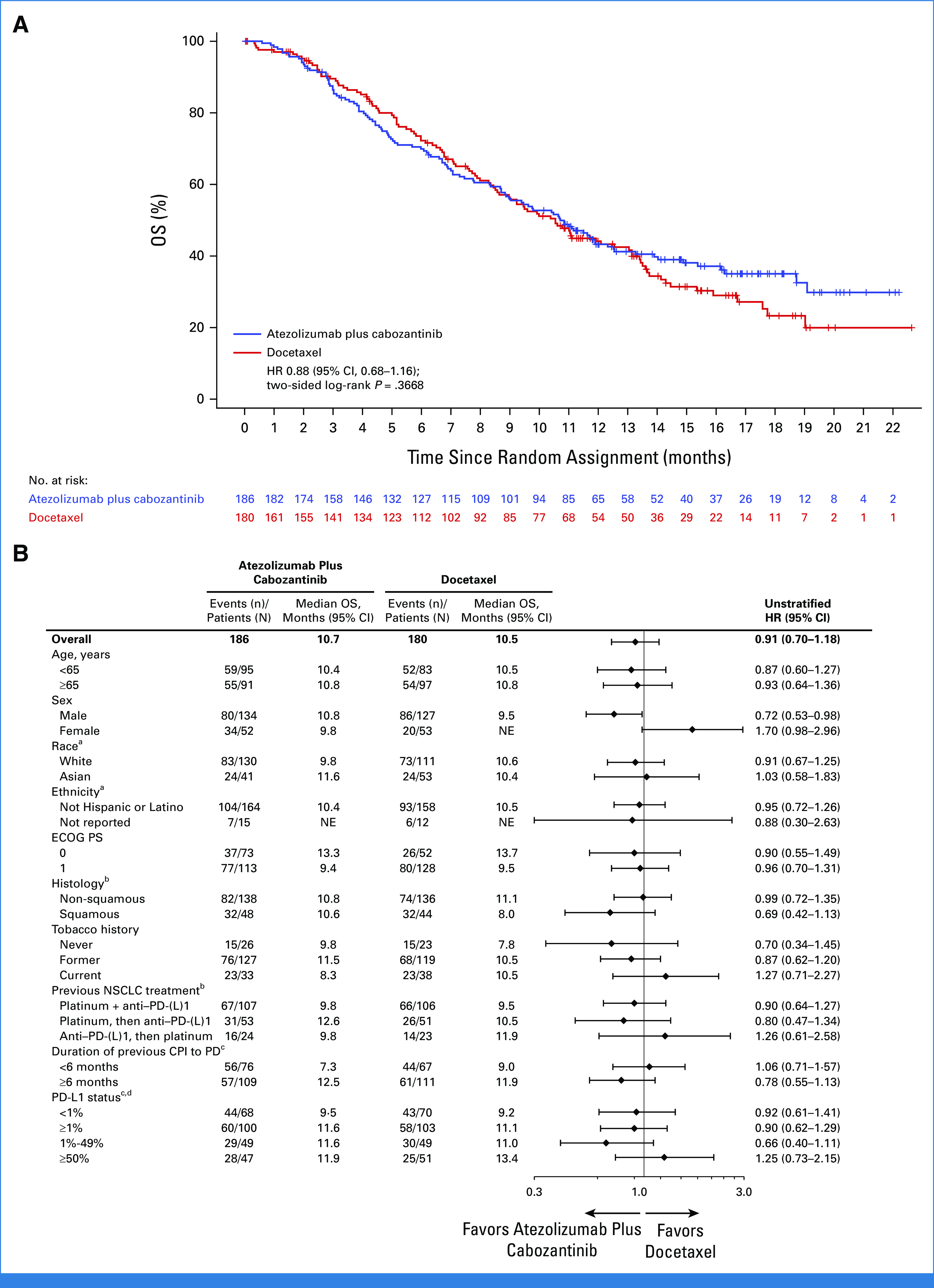
One hundred eighty-six patients were assigned atezolizumab plus cabozantinib, and 180 docetaxel. Minimum OS follow-up was 10.9 months. Median OS was 10.7 months (95% CI, 8.8 to 12.3) with atezolizumab plus cabozantinib and 10.5 months (95% CI, 8.6 to 13.0) with docetaxel (stratified hazard ratio [HR], 0.88 [95% CI, 0.68 to 1.16]; = .3668). Median progression-free survival was 4.6 months (95% CI, 4.1 to 5.6) and 4.0 months (95% CI, 3.1 to 4.4), respectively (stratified HR, 0.74 [95% CI, 0.59 to 0.92]). Serious adverse events (AEs) occurred in 71 (38.4%) patients receiving atezolizumab plus cabozantinib and 58 (34.7%) receiving docetaxel. Grade 3/4 treatment-related AEs occurred in 73 (39.5%) patients receiving atezolizumab plus cabozantinib and 58 (34.7%) receiving docetaxel. Grade 5 AEs occurred in 14 (7.6%) and 10 (6.0%) patients in the atezolizumab plus cabozantinib and docetaxel arms, respectively (treatment-related in four [2.2%] and one [0.6%], respectively).
Atezolizumab plus cabozantinib after disease progression following anti-PD-L1/PD-1 immunotherapy and platinum-containing chemotherapy for metastatic NSCLC did not improve OS compared with docetaxel. Safety was consistent with known profiles of these agents.
尽管检查点抑制剂改善了非小细胞肺癌(NSCLC)的一线治疗,但对于那些疾病没有反应或在抗 PD-L1/PD-1 免疫治疗后疾病进展的患者,仍存在治疗需求。CONTACT-01(ClinicalTrials.gov 标识符:NCT04471428)评估了阿特珠单抗联合卡博替尼与多西他赛在接受抗 PD-L1/PD-1 和含铂化疗联合或序贯治疗后疾病进展的转移性 NSCLC 患者中的疗效。
这是一项多中心、开放标签、III 期试验,按 1:1 比例随机分配患者接受阿特珠单抗 1200mg 静脉注射,每 3 周(q3w)一次,加卡博替尼 40mg 口服,每日一次,或多西他赛 75mg/m2 静脉注射,每 3 周一次。主要终点是总生存期(OS)。
186 名患者被分配接受阿特珠单抗加卡博替尼治疗,180 名患者接受多西他赛治疗。最小 OS 随访时间为 10.9 个月。阿特珠单抗加卡博替尼组的中位 OS 为 10.7 个月(95%CI,8.8 至 12.3),多西他赛组为 10.5 个月(95%CI,8.6 至 13.0)(分层风险比[HR],0.88 [95%CI,0.68 至 1.16];=.3668)。中位无进展生存期分别为 4.6 个月(95%CI,4.1 至 5.6)和 4.0 个月(95%CI,3.1 至 4.4)(分层 HR,0.74 [95%CI,0.59 至 0.92])。阿特珠单抗加卡博替尼组有 71 例(38.4%)和多西他赛组有 58 例(34.7%)发生严重不良事件(AE)。阿特珠单抗加卡博替尼组有 73 例(39.5%)和多西他赛组有 58 例(34.7%)发生 3/4 级治疗相关 AE。阿特珠单抗加卡博替尼组和多西他赛组各有 14 例(7.6%)和 10 例(6.0%)患者发生 5 级 AE(治疗相关分别为 2.2%和 0.6%)。
在抗 PD-L1/PD-1 免疫治疗和含铂化疗治疗转移性 NSCLC 疾病进展后,阿特珠单抗联合卡博替尼并未改善 OS,与多西他赛相比。安全性与这些药物的已知特征一致。