Wronski Marie-Louis, Kuja-Halkola Ralf, Hedlund Elin, Martini Miriam I, Lichtenstein Paul, Lundström Sebastian, Larsson Henrik, Taylor Mark J, Micali Nadia, Bulik Cynthia M, Dinkler Lisa
Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Neuroendocrine Unit, Department of Medicine, Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA.
medRxiv. 2024 Mar 15:2024.03.10.24304003. doi: 10.1101/2024.03.10.24304003.
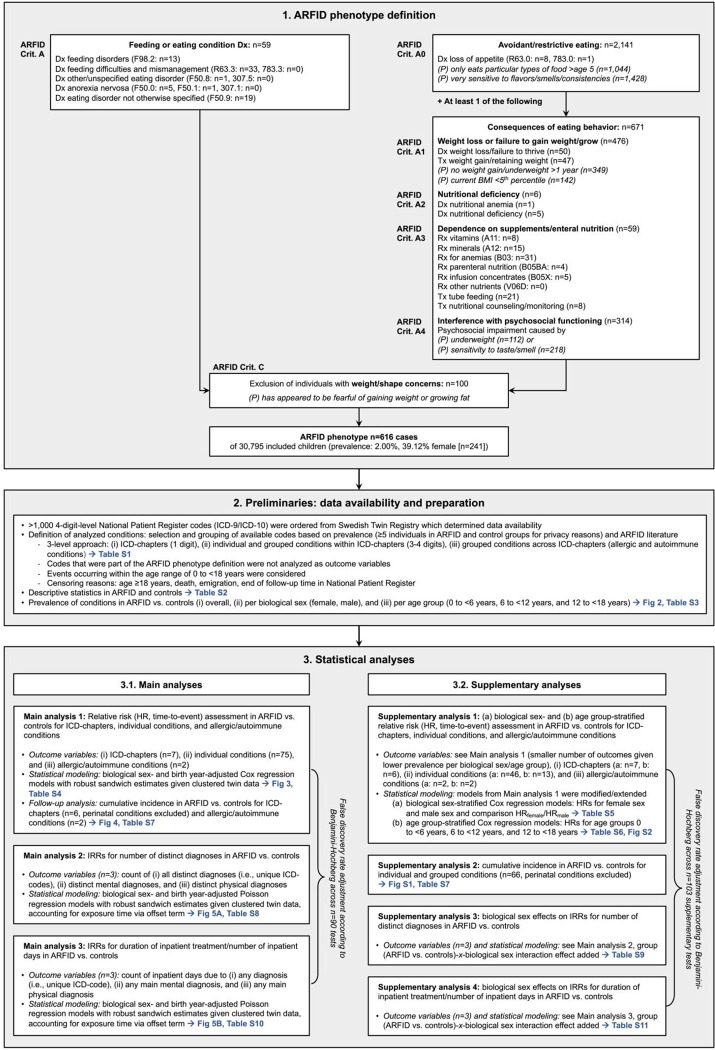
Avoidant restrictive food intake disorder (ARFID) is a feeding and eating disorder, characterized by limited variety and/or quantity of food intake impacting physical health and psychosocial functioning. Children with ARFID often present with a range of psychiatric and somatic symptoms, and therefore consult various pediatric subspecialties; large-scale studies mapping comorbidities are however lacking. To characterize health care needs of people with ARFID, we systematically investigated ARFID-related mental and somatic conditions in 616 children with ARFID and >30,000 children without ARFID.
In a Swedish twin cohort, we identified the ARFID phenotype in 6-12-year-old children based on parent-reports and register data. From >1,000 diagnostic ICD-codes, we specified mental and somatic conditions within/across ICD-chapters, number of distinct per-person diagnoses, and inpatient treatment days between birth and 18 birthday (90 outcomes). Hazard ratios (HR) and incidence rate ratios (IRR) were calculated.
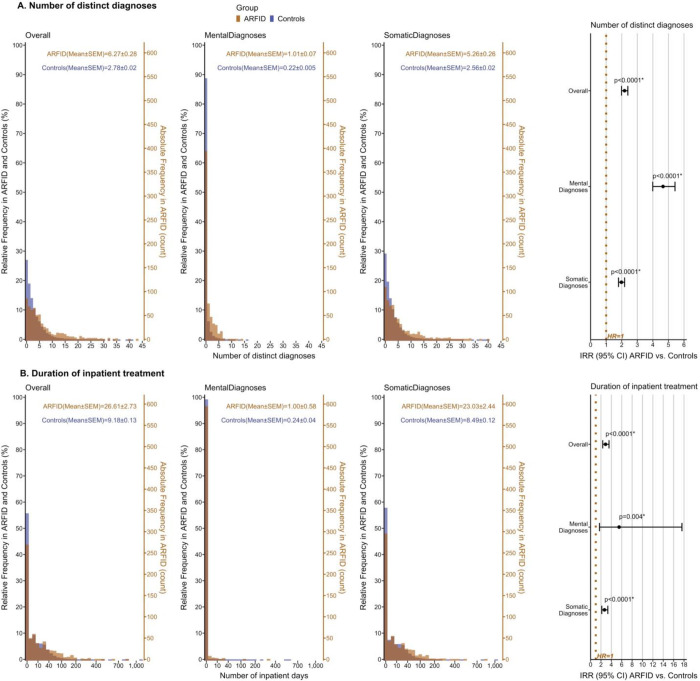
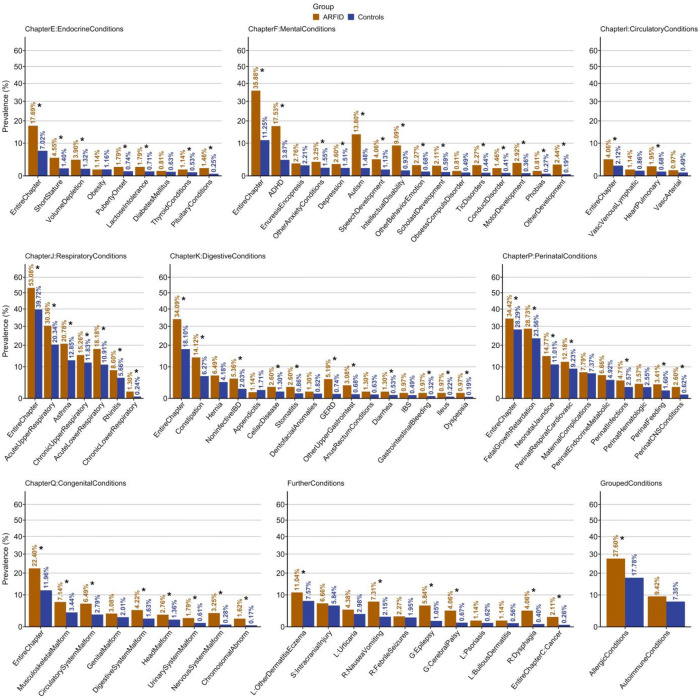
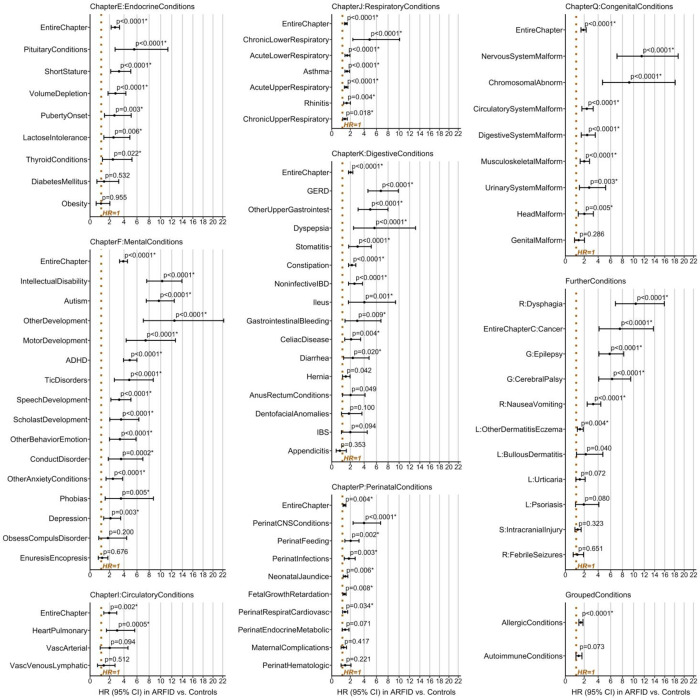
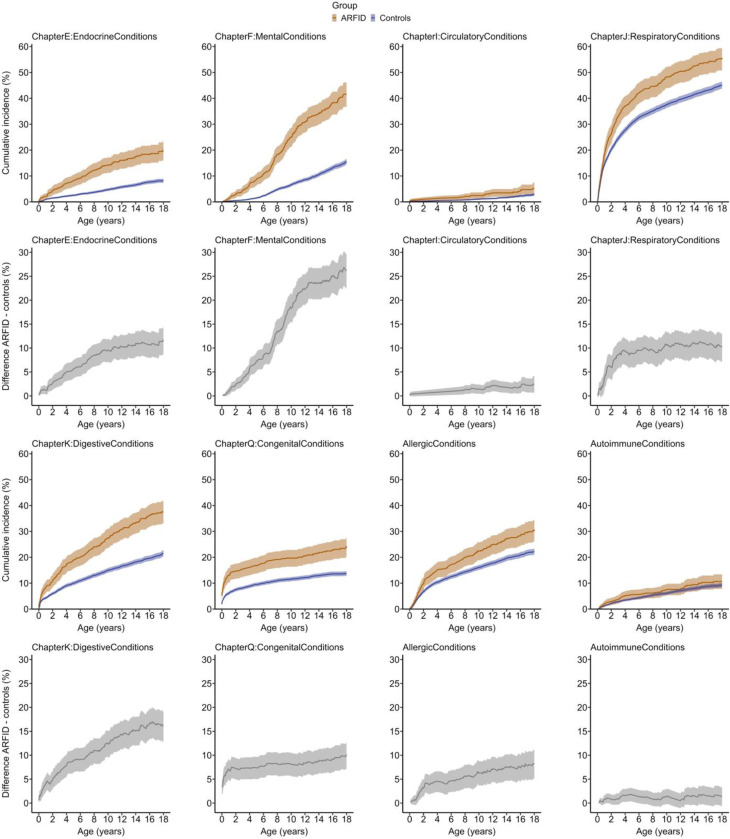
Relative risks of neurodevelopmental, gastrointestinal, endocrine/metabolic, respiratory, neurological, and allergic disorders were substantially increased in ARFID (e.g., autism HR[CI]=9.7[7.5-12.5], intellectual disability 10.3[7.6-13.9], gastroesophageal reflux disease 6.7[4.6-9.9], pituitary conditions 5.6[2.7-11.3], chronic lower respiratory diseases 4.9[2.4-10.1], epilepsy 5.8[4.1-8.2]). ARFID was not associated with elevated risks of autoimmune illnesses and obsessive-compulsive disorder. Children with ARFID had a significantly higher number of distinct mental diagnoses (IRR[CI]=4.7[4.0-5.4]) and longer duration of hospitalizations (IRR[CI]=5.5[1.7-17.6]) compared with children without ARFID. Children with ARFID were diagnosed earlier with a mental condition than children without ARFID. No sex-specific differences emerged.
This study yields the broadest and most detailed evidence of co-existing mental and somatic conditions in the largest sample of children with ARFID to date. Findings suggest a complex pattern of health needs in youth with ARFID, underscoring the critical importance of attention to the illness across all pediatric specialties.
Fredrik and Ingrid Thurings Foundation, Mental Health Foundation.
回避性限制性食物摄入障碍(ARFID)是一种进食障碍,其特征是食物摄入量的种类和/或数量有限,影响身体健康和心理社会功能。患有ARFID的儿童常伴有一系列精神和躯体症状,因此会咨询多个儿科亚专业;然而,缺乏对共病情况进行全面分析的大规模研究。为了明确ARFID患者的医疗需求,我们系统地调查了616名患有ARFID的儿童和30000多名未患ARFID的儿童中与ARFID相关的精神和躯体疾病。
在一个瑞典双胞胎队列中,我们根据家长报告和登记数据,在6至12岁的儿童中确定ARFID表型。从1000多个诊断性国际疾病分类(ICD)编码中,我们明确了ICD各章节内/各章节间的精神和躯体疾病、每人不同诊断的数量,以及出生至18岁生日期间的住院天数(90项结果)。计算风险比(HR)和发病率比(IRR)。
ARFID患者中神经发育、胃肠道、内分泌/代谢、呼吸、神经和过敏性疾病的相对风险大幅增加(例如,自闭症HR[CI]=9.7[7.5 - 12.5],智力残疾10.3[7.6 - 13.9],胃食管反流病6.7[4.6 - 9.9],垂体疾病5.6[2.7 - 11.3],慢性下呼吸道疾病4.9[2.4 - 10.1],癫痫5.8[4.1 - 8.2])。ARFID与自身免疫性疾病和强迫症风险升高无关。与未患ARFID的儿童相比,患有ARFID的儿童有明显更多不同的精神诊断(IRR[CI]=4.7[4.0 - 5.4])和更长的住院时间(IRR[CI]=5.5[1.7 - 17.6])。患有ARFID的儿童比未患ARFID的儿童更早被诊断出患有精神疾病。未发现性别差异。
本研究在迄今为止最大规模的ARFID儿童样本中,得出了关于共存精神和躯体疾病最广泛、最详细的证据。研究结果表明,患有ARFID的青少年存在复杂的健康需求模式,凸显了所有儿科亚专业关注该疾病的至关重要性。
弗雷德里克和英格丽德·图林斯基金会、心理健康基金会。