Lee Hyun Woo, Lee Jung-Kyu, Kim Youlim, Jang An-Soo, Hwang Yong Il, Lee Jae Ha, Jung Ki-Suck, Yoo Kwang Ha, Yoon Hyoung Kyu, Kim Deog Kyeom
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, South Korea.
Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Konkuk University Hospital, School of Medicine, Konkuk University, Seoul, South Korea.
Heliyon. 2024 Mar 12;10(7):e27683. doi: 10.1016/j.heliyon.2024.e27683. eCollection 2024 Apr 15.
Different progressions or prognoses of chronic obstructive pulmonary disease (COPD) have been reported according to structural abnormalities based on chest computed tomography (CT). This study aimed to investigate whether different structural abnormalities independently affect annual lung function changes and clinical prognosis in patients with COPD.
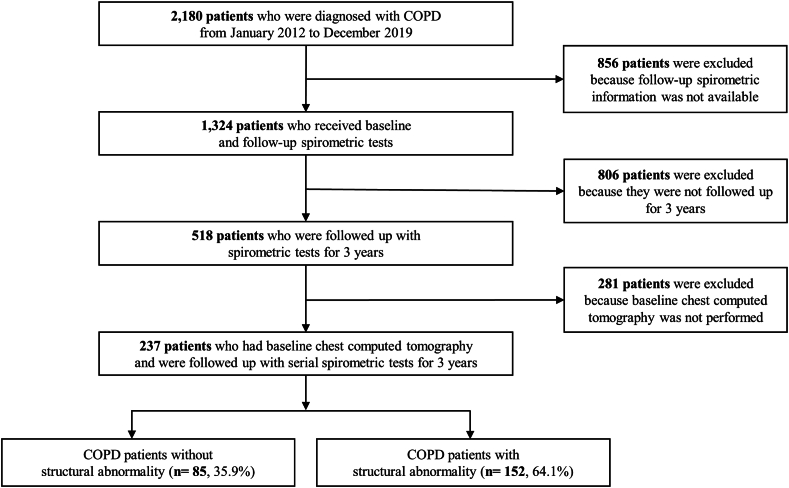
This longitudinal multicenter observational study was conducted using the KOCOSS cohort (NCT02800499) database in Korea from January 2012 to December 2019. For COPD patients with chest CT findings at baseline enrolment and longitudinal spirometric data, annual forced expiratory volume in 1 s (FEV) decline rate (mL/year) and clinical outcomes were compared according to structural abnormalities, including emphysema, bronchiectasis (BE), and tuberculosis-destroyed lung (TDL). We estimated the adjusted annual FEV changes using a mixed-effect linear regression model.
Among the enrolled 237 patients, 152 showed structural abnormalities. Emphysema, BE, and TDL were observed in 119 (78.3%), 28 (18.4%), and 27 (17.8%) patients, respectively. The annual decline in FEV was faster in COPD patients with structural abnormalities than those without (β = -70.6 mL/year, P-value = 0.039). BE/TDL-dominant or emphysema-dominant structural abnormality contributed to an accelerated annual FEV decline compared to no structural abnormality (BE/TDL-dominant, β = -103.7 mL/year, P-value = 0.043; emphysema-dominant, β = -84.1 mL/year, P-value = 0.018). Structural abnormalities made no significant differences in acute exacerbation rate and mortality.
The lung function decline rate in COPD differed according to structural abnormalities on CT. These findings may suggest that more focus should be placed on earlier intervention or regular follow-up with spirometry in COPD patients with BE or TDL on chest CT.
根据胸部计算机断层扫描(CT)显示的结构异常,慢性阻塞性肺疾病(COPD)有不同的进展或预后情况。本研究旨在调查不同的结构异常是否独立影响COPD患者的年度肺功能变化和临床预后。
本纵向多中心观察性研究使用了韩国KOCOSS队列(NCT02800499)数据库,时间跨度为2012年1月至2019年12月。对于在基线入组时有胸部CT检查结果及纵向肺功能数据的COPD患者,根据包括肺气肿、支气管扩张(BE)和结核毁损肺(TDL)在内的结构异常情况,比较每年1秒用力呼气量(FEV)下降率(毫升/年)和临床结局。我们使用混合效应线性回归模型估计调整后的年度FEV变化。
在纳入的237例患者中,152例显示有结构异常。分别在119例(78.3%)、28例(18.4%)和27例(17.8%)患者中观察到肺气肿、BE和TDL。有结构异常的COPD患者FEV的年度下降速度比无结构异常的患者更快(β = -70.6毫升/年,P值 = 0.039)。与无结构异常相比,以BE/TDL为主或肺气肿为主的结构异常导致年度FEV下降加速(以BE/TDL为主,β = -103.7毫升/年,P值 = 0.043;以肺气肿为主,β = -84.1毫升/年,P值 = 0.018)。结构异常在急性加重率和死亡率方面无显著差异。
COPD患者的肺功能下降率因CT上的结构异常而异。这些发现可能表明,对于胸部CT显示有BE或TDL的COPD患者,应更加注重早期干预或定期进行肺功能检查随访。